
The Health Transition That Begins Long Before Most Women Realise
Perimenopause symptoms and lifestyle is a conversation that most women are never invited into until they are already in the middle of the transition, confused, symptomatic, and wondering why nobody told them this was coming. Perimenopause, the years of hormonal transition preceding the final menstrual period, can begin as early as the mid-30s and typically spans between four and ten years. The vast majority of women have no idea it has started until the symptoms become impossible to ignore.
I have worked with women in their late 30s and early 40s who came to me convinced that something was seriously wrong: unexpected weight gain that was not responding to diet and exercise, sleep that had inexplicably deteriorated, mood changes that were affecting their relationships and work, irregular periods after years of clockwork cycles, and a general sense of feeling unlike themselves that no GP appointment had adequately explained. In the majority of cases, perimenopause was the thread connecting all of these experiences. Not a single, manageable event. A multi-year hormonal transition that nobody had prepared them for.
This article is the article I wish existed for every woman entering her mid-to-late 30s. It explains what perimenopause is, when it typically begins, what hormonal changes are driving the symptoms, and what the evidence supports for managing this transition proactively through lifestyle. Because the window for intervention during perimenopause is the most important and most consistently missed opportunity in women's health.
What Perimenopause Actually Is and When It Begins
Perimenopause is the transitional phase during which the ovaries gradually reduce their production of oestrogen and progesterone, leading eventually to the cessation of menstruation. Menopause itself is defined as twelve consecutive months without a menstrual period, at which point perimenopause has ended. The average age of menopause in the UK is 51, which means that perimenopause typically begins in the mid-to-late 40s for most women, but in a meaningful proportion it begins in the late 30s or early 40s (1).
Early perimenopause is frequently unrecognised because the initial hormonal changes are subtle and the symptoms are easily attributed to other causes: work stress, poor sleep, being busy, getting older. The first hormonal shift in perimenopause is typically a decline in progesterone, which occurs before oestrogen begins to fall. Because progesterone is the calming, sleep-supporting, mood-stabilising counterpart to oestrogen, its early decline produces symptoms that include disrupted sleep, increased anxiety, heavier or more irregular periods, and worsening PMS. These symptoms often precede any change in oestrogen levels and therefore any change in the standard blood tests that GPs typically use to assess menopausal status (2).
As perimenopause progresses, oestrogen begins to fluctuate erratically rather than declining smoothly. This fluctuation, which can produce surges above previous normal levels as well as drops below it, is responsible for the wide variability in perimenopausal symptoms and their unpredictability. Hot flushes during a surge, brain fog during a trough, increased libido one week and reduced the next. The erratic nature of oestrogen in perimenopause makes this phase hormonally more complex than menopause itself, when oestrogen simply remains low.
Top Tip
If you are in your late 30s or 40s and experiencing any combination of disrupted sleep, increased anxiety, irregular periods, unexplained weight gain around the middle, worsening PMS, reduced libido, brain fog, joint pain, or changes in how you respond to exercise and food, perimenopause is a legitimate and worthwhile avenue to explore with your GP. Ask specifically for FSH, LH, and oestradiol blood tests, and request them on day 2 to 5 of your cycle if you are still having periods. A single normal result does not rule out perimenopause, as oestrogen fluctuates significantly in this phase.
The Perimenopause Hormonal Timeline
Understanding the trajectory of oestrogen and progesterone across the perimenopausal transition is genuinely useful for contextualising the symptom experience. The diagram below maps the typical pattern, though individual variation is significant.
THE PERIMENOPAUSE HORMONAL TRANSITION
What Is Happening and When
01
Early Perimenopause
Late 30s to Early 40s
What is happening
Progesterone begins to fall. Oestrogen still normal but may fluctuate.
Symptoms
Worsening PMS, disrupted sleep, increased anxiety, heavier periods. Often missed at diagnosis.
02
Mid Perimenopause
Mid to Late 40s
What is happening
Oestrogen fluctuating erratically — peaks and troughs. Progesterone low.
Symptoms
Irregular cycles, hot flushes, brain fog, joint pain, weight gain, mood instability, sleep disruption worsens. Most symptomatic phase.
03
Late Perimenopause
Final 1–2 Years Before Menopause
What is happening
Oestrogen declining more consistently. Periods becoming infrequent. Progesterone very low.
Symptoms
Genitourinary symptoms emerge (dryness, urgency), hot flushes may increase, bone loss accelerates. HRT most effective if started here.
04
Menopause
12 Months No Period
What is happening
Oestrogen stable at a new lower baseline. Progesterone negligible.
Symptoms
May ease as hormones stabilise. Cardiovascular risk increases. Bone loss ongoing. Lifestyle foundations most critical now.
05
Post-Menopause
Ongoing
What is happening
Oestrogen consistently low. Cardiovascular and bone protection both reduced.
Symptoms
Long-term health focus: muscle, bone, cardiovascular, metabolic. What was built or neglected in perimenopause now becomes apparent.
The Symptoms of Perimenopause and Their Physiological Causes
Perimenopause produces a wide range of symptoms that affect virtually every body system. Understanding the mechanism behind each symptom is both practically useful and psychologically valuable: knowing that your symptoms have a clear hormonal explanation reframes them from personal failure to physiological process.
Perimenopause Symptoms — Cause and Lifestyle Intervention
| Symptom | Physiological Cause | Evidence Strength | Primary Lifestyle Intervention |
|---|---|---|---|
| Weight gain, especially around the middle | Falling oestrogen reduces fat redistribution away from visceral depots. Falling progesterone increases cortisol sensitivity. Metabolic rate slows as muscle mass falls. | Strong | Resistance training plus protein-rich nutrition. Manage cortisol. Reduce refined carbohydrates. |
| Sleep disruption | Progesterone has GABA-receptor activity supporting sleep. Its decline disrupts sleep architecture. Oestrogen fluctuation and hot flushes further fragment sleep. | Strong | Sleep hygiene protocol. Consistent wake time. Cool bedroom. Magnesium. Discuss HRT with GP if severe. |
| Hot flushes and night sweats | Oestrogen fluctuation disrupts the hypothalamic thermostat, triggering vasodilation and sweating at narrower temperature thresholds. | Strong for HRT. Moderate for lifestyle | Avoid triggers: alcohol, caffeine, spicy food, hot drinks. Cooling layers. Phytoestrogens may reduce frequency. Discuss HRT with GP. |
| Mood changes, anxiety, low mood | Oestrogen modulates serotonin, dopamine, and GABA pathways. Its fluctuation directly affects mood regulation. Sleep deprivation compounds the effect. | Strong | Resistance training (BDNF and endorphin release). Adequate sleep. Magnesium. Omega 3. Manage overall stress load. |
| Brain fog, poor concentration | Oestrogen supports neuronal function and cerebral blood flow. Its fluctuation impairs working memory, processing speed, and word retrieval. | Moderate | Exercise (increases BDNF). Adequate sleep. Omega 3 and DHA for neurological health. Manage cognitive load. |
| Joint pain and stiffness | Oestrogen has anti-inflammatory properties in connective tissue. Its decline increases inflammatory sensitivity in tendons, ligaments, and joints. | Moderate | Resistance training to strengthen surrounding musculature. Anti-inflammatory nutrition. Omega 3. Adequate hydration. Movement over rest. |
| Irregular periods, heavier bleeding | Erratic oestrogen and falling progesterone produce anovulatory cycles where the endometrium builds without the normal shedding trigger. | Moderate | GP assessment to rule out other causes. Iron intake critical if periods are heavy. Progesterone supplementation via HRT if clinically appropriate. |
| Reduced libido | Testosterone, oestrogen, and progesterone all contribute to libido. The perimenopausal decline in all three, combined with sleep disruption and mood changes, reduces sexual desire. | Moderate | Address sleep, mood, and stress as foundations. Discuss testosterone therapy with GP or menopause specialist if libido is significantly impaired. |
No woman experiences all of these symptoms. No two women experience perimenopause identically. But all of these symptoms have a legitimate hormonal mechanism. If you are experiencing several of them together, this is not anxiety, not burnout, and not simply ageing. It is perimenopause, and it is manageable.
Why the Perimenopausal Window Is the Most Important and Most Missed in Women's Health
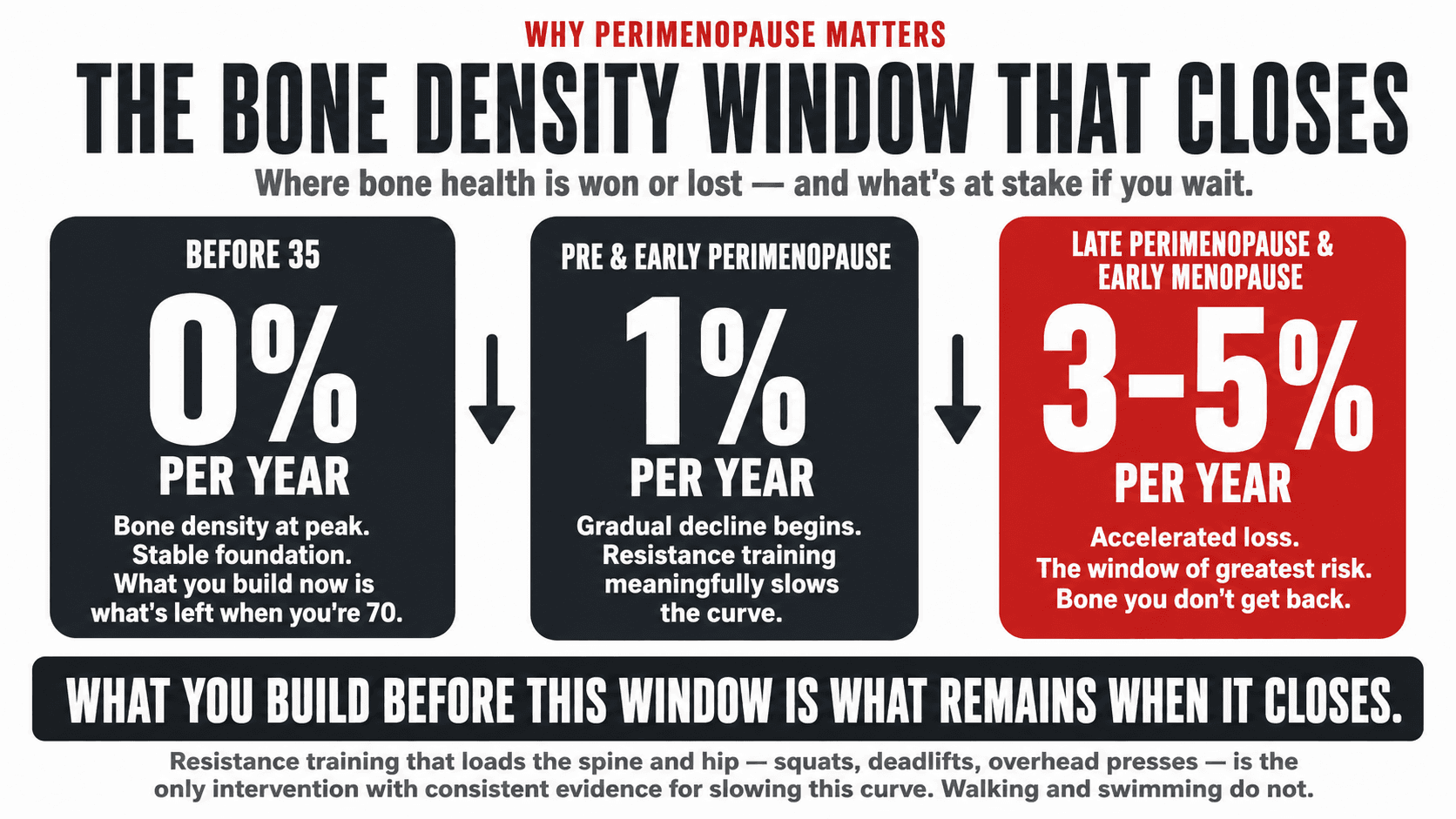
The stakes of perimenopause are not limited to the years of the transition itself. The body composition, muscle mass, bone density, cardiovascular health markers, and metabolic profile that a woman carries into menopause are largely determined by the choices and circumstances of her perimenopausal years. And because perimenopause can span a decade, the opportunity is substantial.
Bone density loss accelerates in the final two years of perimenopause and the first two years of menopause, with women potentially losing three to five percent of bone density per year during this window, compared to approximately one percent per year in the years before (3). The bone density that a woman has built through resistance training and adequate calcium intake before this acceleration begins directly determines how much she has to lose from before serious fracture risk emerges. Women who enter this window with low bone density reserves because they have not trained and have not eaten adequately for bone health are at a significant disadvantage that is very difficult to recover from.
Muscle mass begins to decline more rapidly in perimenopause as the anabolic effect of oestrogen on muscle tissue is withdrawn. This process, known as menopause-related sarcopenia, produces progressive loss of muscle mass and strength that compounds the metabolic slowdown, worsens insulin resistance, increases falls risk, and accelerates the body composition changes that most women find most distressing. Each year of perimenopause without adequate resistance training is a year of preventable muscle loss (4).
The women who navigate perimenopause best are not the ones with the easiest symptom profiles. They are the ones who understood what was happening early and who invested in the lifestyle foundations that protect muscle, bone, and metabolic health during the transition. The difference between these women and those who did not is not genetic. It is informational and behavioural. This article is the information. The behaviour follows from it.
Top Tip
If you are in your late 30s or 40s and have not yet had a DEXA scan to assess bone density, and you have not established a resistance training habit, these are the two most important health investments you can make in this period. A DEXA scan costs approximately £100 to £150 privately in the UK and takes twenty minutes. The information it provides about your bone health starting position is genuinely actionable and worth having before the accelerated bone loss window begins.

Resistance Training in Perimenopause: The Most Important Intervention
The evidence for resistance training in perimenopause is specific, robust, and consistently points in the same direction. Three to four sessions per week of progressive resistance training centred on compound movements builds and preserves the muscle mass that oestrogen is no longer fully protecting, improves insulin sensitivity at a time when it is deteriorating, supports bone density at the site of greatest fracture risk, reduces hot flush frequency and severity, improves mood and sleep quality, and reduces the visceral fat accumulation that accelerates as oestrogen declines (5). There is no pharmaceutical intervention with this breadth of benefit, and no combination of supplements that comes close.
The approach to training in perimenopause should not be fundamentally different from the approach at any other stage. Compound movements, progressive overload, adequate volume, and sufficient recovery are the principles. What may shift is the awareness of recovery needs: some women in perimenopause find that they require slightly more recovery between high-intensity sessions, and that the relationship between training stress and recovery is more sensitive than it was in their 30s. This is not a reason to train less. It is a reason to structure training with slightly more deliberate recovery built in.
One specific consideration worth noting is that very high-intensity training performed at high frequency in an already-stressed hormonal environment can elevate cortisol in a way that worsens rather than improves perimenopausal symptoms. The approach I recommend is high-effort compound resistance training with adequate inter-session recovery, complemented by moderate-intensity cardiovascular work such as walking, cycling, or swimming, rather than daily high-intensity classes.
Top Tip
If you are new to resistance training and entering perimenopause, starting now produces measurable benefits within three to six months. If you have been training consistently for years, continuing with your established programme with appropriate modifications as your recovery needs evolve is the best position to be in. The worst position is stopping training because symptoms are making exercise feel harder. Symptoms are exactly the reason to continue.
Nutrition in Perimenopause: The Evidence-Based Priorities
Nutritional requirements shift meaningfully in perimenopause, and the women who do not adjust their approach often find that food choices that maintained their weight and energy in their 30s no longer work in the same way in their 40s. This is not imagination. It is a physiological reality driven by the hormonal changes described throughout this article.
Protein requirements increase in perimenopause. The anabolic effect of oestrogen on muscle protein synthesis is reduced as oestrogen declines, meaning that the same protein intake that maintained muscle mass in the 30s may be insufficient in the 40s. Research supports a target of 1.6 to 2 grams of protein per kilogram of bodyweight per day for perimenopausal women engaged in resistance training, with some evidence suggesting the upper end of this range is preferable for muscle preservation (6). For plant-based women, tofu, tempeh, edamame, soy protein, pea protein, lentils, chickpeas, and high-leucine plant sources are the foundations of an adequate protein strategy.
Calcium and vitamin D become critical priorities in perimenopause as the accelerated bone loss window approaches. The UK recommended intake for calcium in women over 50 is 700mg per day, but emerging evidence and clinical guidelines increasingly suggest that 1,000 to 1,200mg per day is more appropriate for perimenopausal and postmenopausal women given the rate of oestrogen-related bone loss. Vitamin D supplementation at 1,000 to 2,000IU per day is appropriate for most women in the UK regardless of dietary background, as UK sunlight is insufficient for adequate vitamin D synthesis for most of the year.
Phytoestrogens from soy and flaxseed have attracted genuine research interest for their potential to reduce hot flush frequency and severity. A meta-analysis published in Menopause found that soy isoflavone supplementation reduced hot flush frequency by approximately 26% compared to placebo (7). The effect is modest compared to HRT but is a meaningful addition to the lifestyle toolkit for women experiencing vasomotor symptoms. Dietary phytoestrogens from tofu, tempeh, edamame, soy milk, and flaxseed are safe, nutritionally valuable, and relevant for all women in perimenopause regardless of dietary background.
Magnesium is consistently under-consumed in women and becomes particularly relevant in perimenopause for its role in sleep quality, mood regulation, cortisol management, and bone health. The recommended intake for women is 270mg per day, and the best dietary sources are dark chocolate, pumpkin seeds, almonds, cashews, spinach, avocado, and black beans. A magnesium glycinate supplement of 200 to 400mg taken before bed is one of the most practically effective and well-tolerated additions to a perimenopausal nutrition strategy.
Top Tip
The single most impactful dietary change for most perimenopausal women is increasing protein while reducing refined carbohydrates. More protein preserves muscle mass as oestrogen declines. Less refined carbohydrate reduces the blood glucose volatility that worsens insulin resistance during the transition. These two changes together, applied consistently, address the two most significant nutritional drivers of perimenopausal body composition change. No elimination diet required.

Sleep in Perimenopause: Why It Deteriorates and How to Protect It
Sleep disruption is one of the most universally reported and most functionally damaging symptoms of perimenopause. Progesterone's GABA-receptor activity, which supports sleep initiation and maintenance, is lost as progesterone falls. Oestrogen fluctuation disrupts the sleep architecture further, and hot flushes and night sweats cause fragmented sleep that prevents the deep, restorative phases from completing fully.
The practical sleep protection strategy for perimenopausal women builds on the sleep hygiene foundations that apply universally, with specific additions relevant to hormonal sleep disruption. A consistent wake time seven days per week anchors the circadian rhythm regardless of night-to-night variation in sleep quality. A cool bedroom, between 16 and 18 degrees Celsius, reduces the frequency and severity of hot flush triggered waking. Avoiding alcohol in the evening is particularly important in perimenopause, as alcohol directly suppresses REM sleep and worsens hot flushes through vasodilation.
Magnesium glycinate before bed has good evidence for improving sleep onset and quality through its GABA-receptor activity, partially compensating for the loss of progesterone's sleep-supporting effect. This is a practical, inexpensive, and well-tolerated intervention that I recommend as a starting point before considering pharmaceutical sleep aids.
Top Tip
Track your sleep quality for two to four weeks using a simple morning rating from one to ten alongside noting whether a hot flush or night sweat woke you. This data is useful for identifying patterns and for conversations with your GP about whether HRT is appropriate. Sleep data also gives you objective evidence that the problem is not anxiety or stress alone, which is a distinction that matters for getting the right clinical support.
HRT in Perimenopause: What the Current Evidence Actually Says
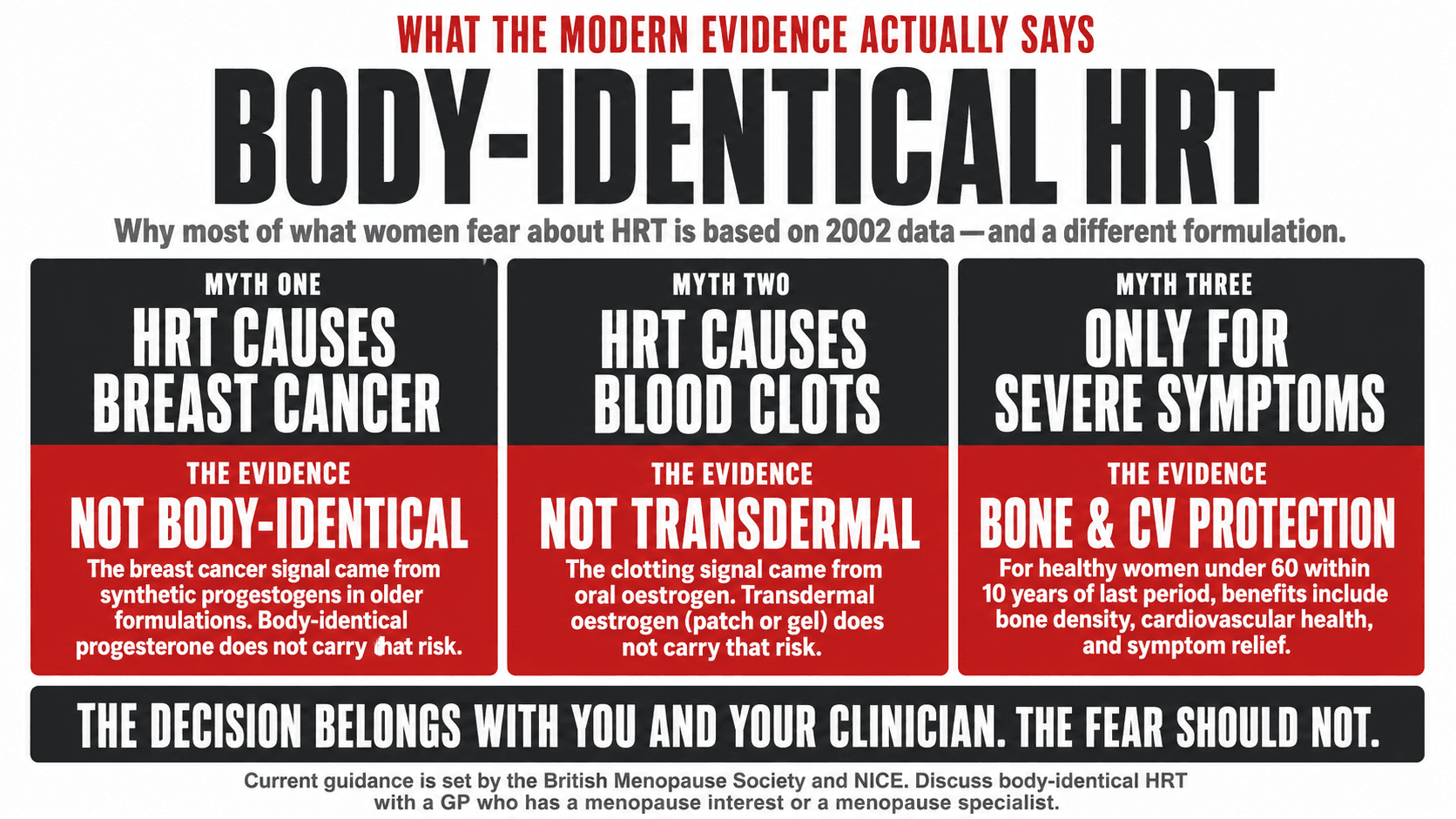
Hormone replacement therapy is one of the most misunderstood, most feared, and most clinically valuable interventions in women's health. The fear of HRT that many women carry was generated substantially by the Women's Health Initiative study published in 2002, which reported increased breast cancer and cardiovascular risk in women using a specific form of combined HRT. The methodology and context of that study have been substantially reanalysed in the decades since, and the clinical guidance on HRT has shifted significantly as a result.
The current position of the British Menopause Society and NICE guidelines is that for healthy women under 60 who are within ten years of their last period, the benefits of HRT for symptom management, bone protection, and cardiovascular health generally outweigh the risks, and that the older, more alarming risk estimates derived from oral conjugated equine oestrogen plus medroxyprogesterone acetate do not apply to modern body-identical HRT formulations (8).
Body-identical HRT, which uses oestrogen and progesterone that are molecularly identical to the hormones the ovaries produce, is the formulation that most menopause specialists now recommend. Transdermal oestrogen, delivered via patch or gel, does not carry the elevated venous thromboembolism risk associated with oral oestrogen. Body-identical progesterone does not carry the elevated breast cancer risk associated with synthetic progestogens.
This is not a recommendation that every perimenopausal woman should take HRT. It is a recommendation that every perimenopausal woman should have an informed, current, evidence-based conversation with a GP or menopause specialist about whether it is appropriate for them. The decision belongs with the individual and their clinician. My role is to ensure that the lifestyle foundations are as strong as possible, and to make sure that no woman approaches that conversation with a fear of HRT based on outdated information.
Top Tip
If you want to discuss HRT with your GP, ask specifically to see a GP with a menopause interest, or ask for a referral to a menopause clinic. Not all GPs are equally trained in menopause management, and the quality of the conversation varies significantly. You can also access a private menopause specialist consultation in the UK for around £200 to £300 if you want a dedicated assessment. The British Menopause Society website has a find-a-specialist directory.
YOUR PERIMENOPAUSE ACTION PLAN
Four Quadrants. One Transition.
01
Resistance Training
- 3 to 4 sessions per week
- Compound movements: squats, deadlifts, rows, presses
- Progressive overload: increase load over time
- Adequate recovery: do not train through fatigue daily
- Spinal and hip loading for bone density
- Post-meal walking for insulin sensitivity
02
Nutrition
- Protein: 1.6 to 2g per kg per day
- Calcium: 1,000 to 1,200mg per day
- Vitamin D: 1,000 to 2,000IU supplement daily
- Magnesium: 270mg plus consider glycinate supplement
- Phytoestrogens: tofu, tempeh, flaxseed, edamame
- Reduce refined carbohydrates and alcohol
03
Sleep and Stress
- Consistent wake time seven days per week
- Cool bedroom: 16 to 18 degrees Celsius
- Avoid alcohol, particularly in evenings
- Magnesium glycinate 200 to 400mg before bed
- Manage overall stress and cortisol load
- Deload training weeks every four to six weeks
04
Medical Review
- Ask GP for FSH, LH, oestradiol, thyroid panel
- Request bone density DEXA scan
- Discuss HRT with GP with menopause interest
- Track symptoms for four weeks before appointment
- Explore body-identical HRT if appropriate
- Annual cardiovascular health check from age 45
Perimenopause is a transition, not a decline. Every quadrant of this plan is an active investment in the health and body you carry into menopause and the decades that follow. The earlier you start, the more you accumulate. But it is never too late to begin.
How I Work With Women in Perimenopause
Perimenopause is one of the most significant and most productively manageable transitions in a woman's health journey, and it is one I work with regularly and with particular attention to the hormonal and metabolic context that makes coaching at this stage different from coaching a 28-year-old.
The programme I build for a perimenopausal client accounts for the hormonal environment she is currently navigating: her symptom profile, her recovery capacity, her sleep quality, her stress load, and her nutritional baseline. Resistance training is always the centrepiece. Nutrition is structured around the specific priorities that perimenopause creates. Recovery is treated with the seriousness it deserves at this stage rather than pushed through.
The women I have worked with who engaged with perimenopause proactively, who built their training and nutritional foundations during the transition rather than waiting until the symptoms became overwhelming, entered post-menopause from a position of strength rather than deficit. That is the outcome this work is designed to produce. If you are in perimenopause and ready to navigate it with that level of intention, I am here to help. One-to-one, online globally.
