The obesity health crisis is the single greatest threat to public health in the United Kingdom today, and we are not treating it with anywhere near the urgency it demands. Over the past 50 years, we have waged a remarkably successful public health war against smoking. We banned tobacco advertising. We plastered graphic health warnings on every packet. We prohibited smoking in public places, raised taxes on cigarettes to punitive levels, and funded nationwide campaigns telling people in no uncertain terms that smoking would kill them. And it worked. Smoking rates in the UK have plummeted from over 45 percent of adults in the 1970s to around 12 percent today. That is one of the great public health victories of the modern era.
Meanwhile, obesity has been quietly and relentlessly moving in the opposite direction. In 1993, 15 percent of adults in England were classified as obese. By 2024, that figure had doubled to 30 percent. Two thirds of adults in England are now either overweight or obese (1). Obesity costs the NHS an estimated £6.5 billion per year in direct treatment costs, and the wider economic burden including lost productivity, reduced quality of life, and social care costs is estimated at £98 billion annually (2). These are not abstract numbers. This is a crisis that is shortening lives, overwhelming health services, and draining the economy. And yet, compared to the aggressive, systemic approach we took with smoking, our response to obesity has been timid, fragmented, and wholly inadequate.
Obesity Is Now Killing More People Than Smoking
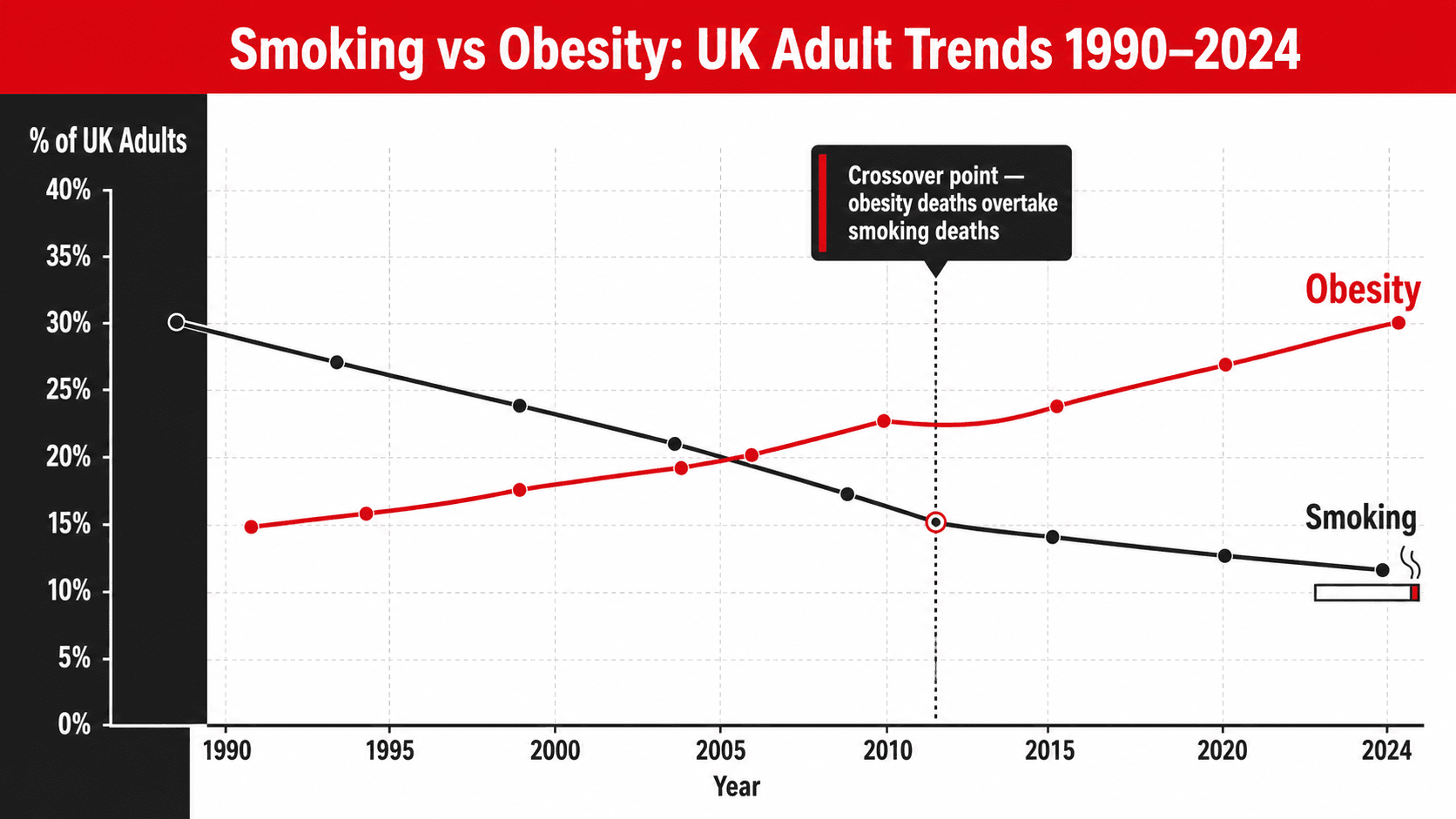
This is not hyperbole. A comparative risk assessment study published in BMC Public Health analysed data from health surveys across England and Scotland from 2003 to 2017. The researchers found that deaths attributable to smoking declined from 23.1 percent of all deaths in 2003 to 19.4 percent in 2017. During the same period, deaths attributable to excess body fat increased from 17.9 percent to 23.3 percent. The crossover point occurred in 2013. Since then, obesity and overweight have been responsible for a greater share of deaths in the UK than smoking (3). Let that figure sit with you. The condition that barely registers on most people’s threat radar is now a bigger killer than the one plastered with skull and crossbones warnings on every shop shelf in the country.
A separate individual-participant data meta-analysis of nearly 4 million people from 189 studies across Europe, North America, East Asia, Australia, and New Zealand confirmed that individuals with a BMI above 25 had a significantly increased risk of dying prematurely, with approximately one in six premature deaths potentially avoidable through maintaining a healthy weight (4). The senior author of that study, Professor Sir Richard Peto of the University of Oxford, stated plainly that obesity is second only to smoking as a cause of premature death in Europe and North America. Given the trajectory of the data, it may not hold that position for long.
Smoking vs Obesity: A Side by Side Comparison
To understand why I believe we need to treat obesity with the same seriousness as smoking, it helps to see the two crises side by side. The parallels are striking, and the differences in our response are damning.
| Smoking | Obesity | |
|---|---|---|
| UK Adult Prevalence | Approximately 12% of adults currently smoke | 30% of adults are obese. 66% are overweight or obese (1) |
| Trend Direction | Declining steadily for decades | Doubled since 1993 and still rising (1) |
| Annual NHS Cost | Estimated at £2.5 billion per year | Estimated at £6.5 billion per year (2) |
| Share of UK Deaths | 19.4% of all deaths in 2017 (3) | 23.3% of all deaths in 2017 (3) |
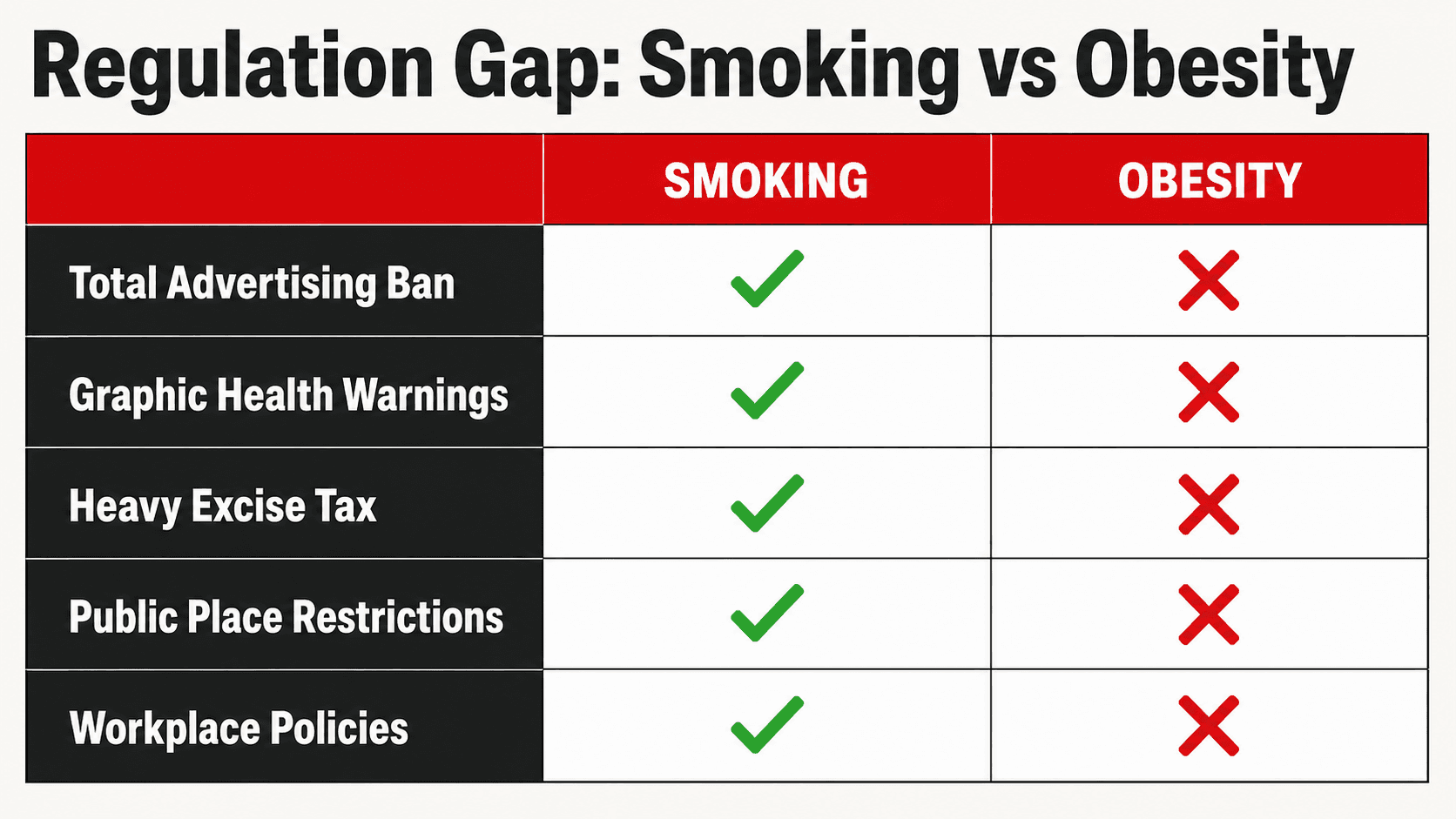
| Advertising Restrictions | Total ban on tobacco advertising since 2003 | Restrictions on HFSS food advertising before 9pm only from October 2025 |
| Packaging Warnings | Graphic health warnings mandatory on all packs | No equivalent health warnings on food packaging |
| Taxation | Heavy excise duties making cigarettes progressively unaffordable | Soft Drinks Industry Levy only. No broader sugar or junk food tax |
| Public Perception | Universally acknowledged as dangerous and socially unacceptable | Often minimised, normalised, or treated as a personal lifestyle choice rather than a health crisis |
| Workplace Policies | Banned in all enclosed workplaces since 2007 | No equivalent policies addressing the food environment in workplaces |
The contrast is stark. We threw everything at smoking and it worked. We have barely scratched the surface with obesity. The food environment in the UK actively promotes overconsumption of cheap, ultra-processed, calorie-dense food at every turn. Supermarkets stack multipack confectionery at the checkout. Fast food outlets cluster in the most deprived communities. Advertising for processed food is everywhere. And the messaging around personal responsibility, while partially valid, has been used as a convenient excuse for governments and the food industry to avoid the kind of systemic, structural interventions that actually moved the needle on smoking.
The Health Consequences of Obesity Are as Severe as Smoking
Obesity is not a cosmetic issue. It is a medical condition that significantly increases the risk of a long list of life-threatening and life-limiting diseases. The World Health Organisation classifies obesity as a chronic, relapsing disease that requires long-term management (5). It is directly associated with type 2 diabetes, cardiovascular disease, hypertension, stroke, non-alcoholic fatty liver disease, obstructive sleep apnoea, osteoarthritis, depression, and at least 13 types of cancer including breast, colon, kidney, and pancreatic cancer (5, 6).
Data from the United States using the National Health and Nutrition Examination Survey found that adults who were obese, currently smoking, and physically inactive had a 231 percent greater rate of dying from all causes compared to those who were normal weight, never smoked, and were physically active (7). The combined clustering of these risk factors advanced the age of death by an estimated 13 years for all-cause mortality. Obesity alone, independent of smoking and inactivity, carried a hazard ratio of 1.51 for cardiovascular disease mortality. This is not a minor inconvenience. This is a condition that is measurably and significantly shortening people’s lives.
I see the consequences of this every week in my coaching practice. I work with clients who arrive with type 2 diabetes, hypertension requiring medication, elevated liver enzymes, joint pain that limits their ability to move, sleep apnoea that leaves them exhausted, and a metabolic profile that puts them at serious risk of a cardiac event. These are not elderly people in poor health. Many of them are in their 30s and 40s. They are professionals, parents, and people in the prime of their working lives who have been slowly, silently damaged by decades of excess body fat. And almost all of them tell me the same thing: nobody ever told them how serious this was.
How Obesity Increases Your Risk: The Numbers
The following table summarises the increased risk of major health conditions associated with obesity, drawn from large-scale epidemiological studies and meta-analyses. These are not worst-case scenarios. These are average population-level risks.
| Health Condition | Increased Risk with Obesity (BMI 30+) |
|---|---|
| Type 2 Diabetes | Risk increased approximately 7-fold compared to normal weight individuals (5) |
| Cardiovascular Disease | 51% increased risk of CVD mortality in obese individuals (7) |
| Hypertension | Obesity is the strongest modifiable risk factor for hypertension. Risk increases progressively with BMI (5) |
| Certain Cancers | Linked to at least 13 cancer types. Obesity is the second biggest preventable cause of cancer in the UK (6) |
| Stroke | Risk increased by 26 to 64% depending on obesity severity (5) |
| Non-Alcoholic Fatty Liver Disease | Present in up to 80 to 90% of individuals with obesity (5) |
| Obstructive Sleep Apnoea | Obesity is present in approximately 60 to 70% of sleep apnoea cases (5) |
| Osteoarthritis | Risk of knee osteoarthritis increases approximately 4-fold with obesity (5) |
| Depression and Mental Health | Obesity is associated with a 55% increased risk of depression (5) |
| All-Cause Premature Death | One in six premature deaths in Europe and North America are attributable to excess weight (4) |
Why Do We Treat Obesity Differently from Smoking
If obesity kills more people than smoking, costs the NHS nearly three times as much, and is associated with an equally devastating list of chronic diseases, why does it not receive the same level of public health intervention? The answer is a combination of political cowardice, commercial interests, cultural normalisation, and a deeply flawed belief that obesity is simply a matter of individual choice.
The food industry is extraordinarily powerful. Ultra-processed food manufacturers spend billions on advertising, lobbying, and product formulation designed to maximise consumption. They have successfully framed the obesity debate as a matter of personal responsibility for decades, deflecting attention from the fact that they have engineered a food environment that makes overconsumption almost inevitable for large sections of the population. This is the same playbook the tobacco industry used for 40 years before regulators finally intervened. The parallels are not subtle.
There is also a cultural dimension. We have normalised overweight and obesity to such an extent that carrying an extra 10, 20, or 30 kilograms of body fat is considered unremarkable. Walk through any town centre in the UK and the visual norm is overweight. When the majority of the population is above a healthy weight, being overweight stops looking abnormal. But statistical normality and biological health are not the same thing. The fact that most people around you are overweight does not mean it is safe. It means the crisis is so widespread that it has distorted our frame of reference entirely.

I want to be very clear about something. Acknowledging that obesity is a serious health crisis is not an attack on anyone’s character, worth, or dignity. People living with obesity deserve compassion, respect, and access to effective support. But compassion does not mean pretending that excess body fat is harmless. It is not. Just as we do not tell a smoker that their habit is fine to protect their feelings, we should not pretend that obesity is without consequence. Honesty, delivered with empathy and paired with genuine help, is the most compassionate response there is.
What Needs to Change at a Structural Level
I am a body transformation coach, not a politician. My arena is the individual. I work with one person at a time, building personalised nutrition and training programmes that address their specific health challenges and goals. But I am also someone who sees the consequences of this crisis up close every single day. And I believe we need structural changes that go far beyond telling people to eat less and move more.
We need comprehensive restrictions on the advertising of ultra-processed food, not just before the 9pm watershed, but across all media platforms with the same rigour applied to tobacco. We need clear, front-of-pack health warnings on food products that are high in sugar, salt, and saturated fat, similar to the approach already adopted in countries like Chile and Mexico. We need a genuine fiscal strategy that makes whole, minimally processed food more affordable and calorie-dense processed food relatively more expensive. The Soft Drinks Industry Levy was a good start but it barely scratches the surface. We need urban planning that prioritises access to green spaces, safe walking and cycling routes, and limits the clustering of fast food outlets in deprived areas. And we need the medical profession to treat obesity with the clinical seriousness it deserves, screening for it proactively, addressing it directly, and offering genuine pathways to evidence-based support.

What You Can Do Right Now as an Individual
While I believe systemic change is essential, I also believe in personal agency. You do not have to wait for government policy to change before you take control of your own health. The same evidence base that demonstrates the scale of the obesity crisis also demonstrates that modest weight loss produces significant health benefits. A reduction of just 5 to 10 percent of body weight is associated with meaningful improvements in blood pressure, blood glucose, HbA1c, cholesterol, liver function, and all-cause mortality risk (8). You do not need to become an athlete. You need to become leaner, stronger, and more metabolically healthy than you are right now.
Start with a moderate, sustainable calorie deficit. Prioritise protein at every meal from whatever sources suit your dietary preferences, whether that is chicken, fish, eggs, tofu, tempeh, seitan, lentils, chickpeas, soy protein, pea protein, or dairy alternatives. Lift weights two to four times per week to build and preserve lean muscle mass. Walk more. Sleep more. Reduce your intake of ultra-processed food and replace it with whole, minimally processed alternatives. Measure your waist circumference and track it alongside your body weight. Get your blood work done and know your fasting glucose, HbA1c, lipid panel, and liver enzymes. Take this as seriously as you would take a cancer screening or a heart check. Because that is exactly what it is.
The Bottom Line
Obesity is a health crisis of the same magnitude as smoking. In the UK, it now contributes to more deaths annually than tobacco. It costs the NHS £6.5 billion a year in direct treatment and the wider economy £98 billion. It is associated with type 2 diabetes, cardiovascular disease, at least 13 types of cancer, and a measurable reduction in lifespan. And yet we have responded with a fraction of the urgency, regulation, and investment that we directed at smoking. That needs to change at a societal level. But it also needs to change at a personal level.
If you are carrying excess body fat, the time to act is now. Not next month, not next year, now. The longer excess weight sits on your body, the greater the cumulative damage to your metabolic health, your joints, your liver, your cardiovascular system, and your quality of life. A structured, evidence-based approach to fat loss under professional guidance is one of the most powerful health interventions available to you. It is more impactful than most medications, more protective than most supplements, and more effective than most things people spend their money on in pursuit of better health.
If you want help, get in touch. I work one-to-one with clients online globally. Whether you eat meat, are vegetarian, vegan, or somewhere in between, whether you are managing diabetes, hypertension, PCOS, or simply want to lose fat and improve your long-term health, I will build a programme that addresses your specific needs with the seriousness they deserve. This is not about aesthetics. This is about your health. And your health is worth fighting for.
Work with Me
Get a personalised coaching plan built around your goals, your schedule, and your life.
Enquire NowReferences
- NHS Digital. Health Survey for England 2024: Adults’ Overweight and Obesity. NHS England. 2025.
- Frontier Economics. The Rising Cost of Obesity in the UK. Tony Blair Institute for Global Change. 2023.
- Ho FK, Celis-Morales C, Gray SR, et al. Changes over 15 years in the contribution of adiposity and smoking to deaths in England and Scotland. BMC Public Health. 2021; 21(1): 169.
- Global BMI Mortality Collaboration. Body-mass index and all-cause mortality: individual-participant-data meta-analysis of 239 prospective studies in four continents. The Lancet. 2016; 388(10046): 776-786.
- World Health Organization. Obesity and Overweight Fact Sheet. WHO. 2024.
- Lauby-Secretan B, Scoccianti C, Loomis D, et al. Body fatness and cancer: viewpoint of the IARC Working Group. New England Journal of Medicine. 2016; 375(8): 794-798.
- Borrell LN, Graham L, Joseph SP. The clustering effects of current smoking status, overweight/obesity, and physical inactivity with all-cause and cause-specific mortality risks in U.S. adults. Preventive Medicine Reports. 2024; 42: 102738.
- Wing RR, Lang W, Wadden TA, et al. Benefits of modest weight loss in improving cardiovascular risk factors in overweight and obese individuals with type 2 diabetes. Diabetes Care. 2011; 34(7): 1481-1486.