
Most people think of body fat as a single entity. You gain it, you lose it, and the number on the scale tells you where you stand. But the reality is far more nuanced than that, and body fat distribution diabetes risk is something that most people never think about until it is too late. Two people can weigh exactly the same, carry the same total body fat percentage, and face completely different health outcomes depending on where that fat is stored. One of them may be metabolically healthy with clean blood work and stable blood sugar. The other may be on the path to insulin resistance, type 2 diabetes, cardiovascular disease, and a host of inflammatory conditions. The difference is not how much fat they carry. It is where their body has chosen to deposit it.
This is not a theoretical concern. This is something I see in my coaching practice regularly. I work with clients who have been told they are fine because their BMI falls within a normal range, yet their waist circumference, blood glucose, and inflammatory markers tell a very different story. I also work with clients who carry more total body fat than the guidelines suggest but store it in places that cause far less metabolic disruption. Understanding body fat distribution is one of the most important and most overlooked pieces of the health and fat loss puzzle. If you are serious about your long term health, about reducing your risk of type 2 diabetes, and about making informed decisions about your body, this article will give you the knowledge to do exactly that.
Not All Body Fat Is Created Equal
Body fat is broadly categorised into two main types based on its location in the body. Subcutaneous fat is the fat stored directly under the skin. It is the fat you can physically pinch on your arms, thighs, hips, and abdomen. Visceral fat, on the other hand, is stored deep inside the abdominal cavity, surrounding your internal organs including the liver, pancreas, and intestines. You cannot see it or pinch it, but it is there, and it behaves in a fundamentally different way to the fat sitting under your skin.
Subcutaneous fat, particularly the fat stored in the lower body around the hips, thighs, and gluteal region, is generally considered metabolically neutral or even protective. Research from the Framingham Heart Study found that subcutaneous abdominal fat was not associated with a linear increase in metabolic risk factors among obese individuals, and in some cases appeared to offer a buffering effect against elevated triglycerides (1). The theory behind this is that subcutaneous fat acts as a safe storage depot for excess energy. When your body has somewhere to put surplus calories without those calories ending up in places they should not be, the metabolic consequences are significantly less severe.
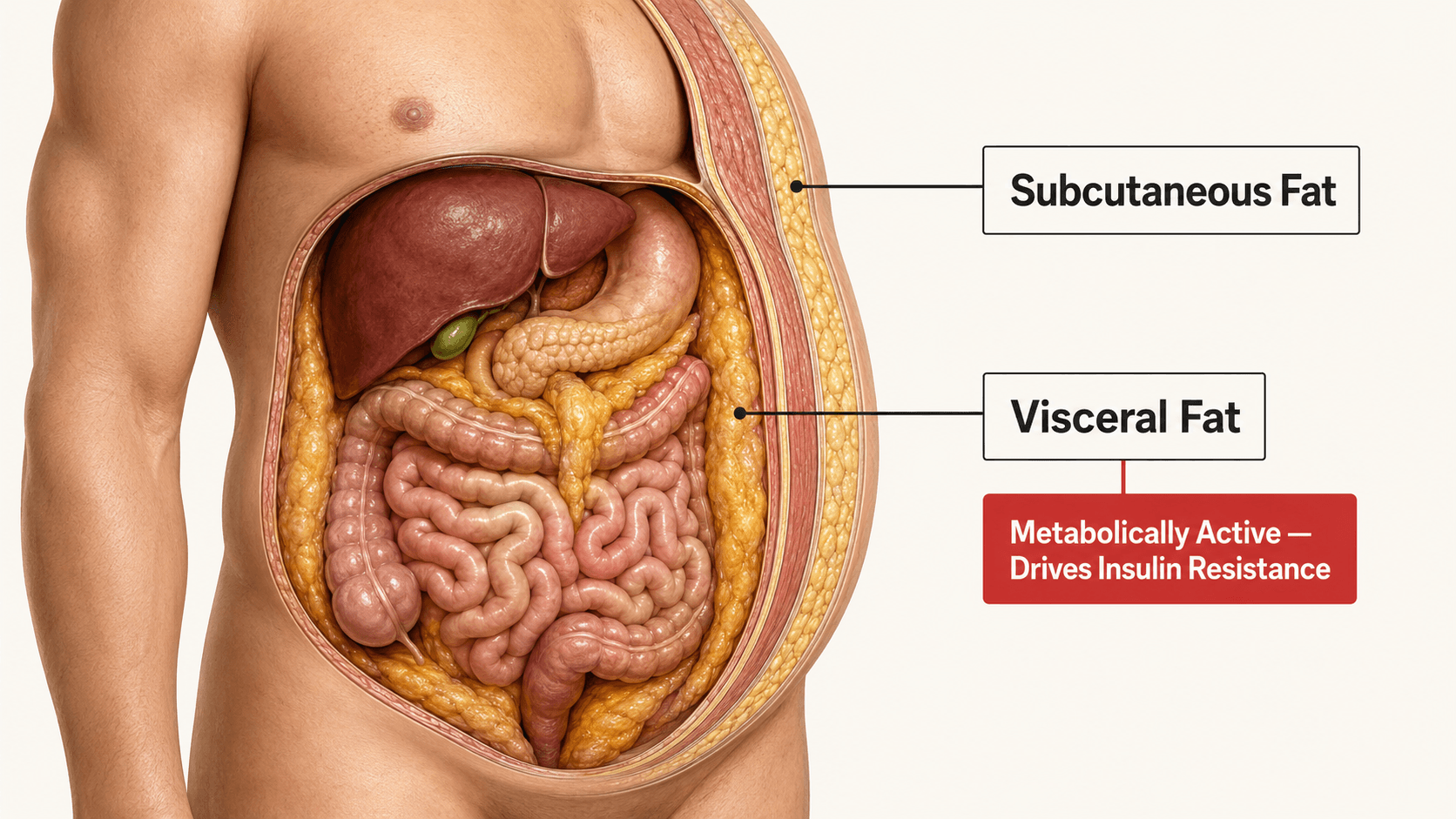
Visceral fat is a different matter entirely. It is metabolically active tissue that functions almost like an endocrine organ, releasing inflammatory cytokines, free fatty acids, and hormones that directly interfere with insulin signalling, liver function, and systemic inflammation (2). Because visceral fat drains directly into the portal vein, the free fatty acids it releases flood the liver, impairing hepatic insulin clearance and driving insulin resistance from the inside out. This is why two people at the same body weight can have vastly different metabolic profiles. The one carrying more visceral fat is at significantly greater risk.
Apple vs Pear: What Your Body Shape Tells You About Your Health
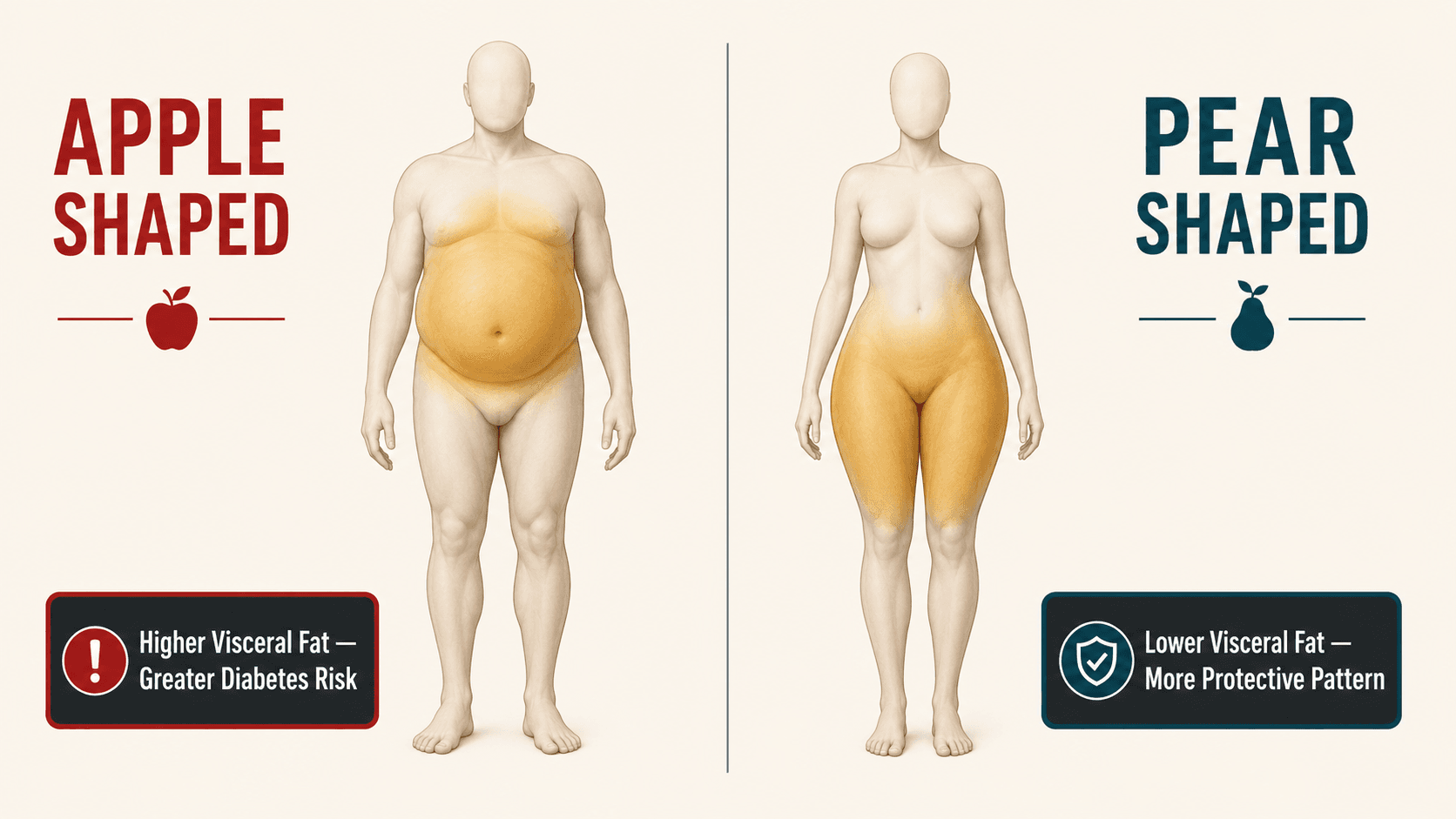
You have probably heard the terms apple shaped and pear shaped used to describe body types. These are not just aesthetic descriptions. They are crude but useful indicators of where your body preferentially stores fat, and they carry very different implications for your metabolic health.
An apple shaped body stores fat predominantly around the midsection, the trunk, and the abdominal cavity. This pattern is strongly associated with higher levels of visceral fat and is far more common in men, although women can and do develop this pattern, particularly after menopause when declining oestrogen levels shift fat distribution away from the hips and towards the abdomen (3). A pear shaped body stores fat predominantly around the hips, thighs, and buttocks, with relatively less abdominal accumulation. This pattern is more common in premenopausal women and is associated with a more favourable metabolic profile.
A comprehensive review published in The Lancet Diabetes and Endocrinology confirmed that an impaired ability to expand subcutaneous fat in the lower body is just as important as a high amount of visceral fat in determining the risk of type 2 diabetes and cardiovascular disease (4). In other words, it is not just about having too much visceral fat. It is also about not having enough capacity in the safer storage depots. When the body runs out of safe places to store surplus energy, the overflow ends up in visceral depots and in ectopic locations such as the liver, the pancreas, and within muscle tissue, all of which accelerate metabolic dysfunction.
| Visceral Fat | Subcutaneous Fat | |
|---|---|---|
| Location | Deep inside the abdominal cavity, surrounding internal organs | Directly under the skin across the body |
| Can You See It? | No. It is hidden internally. You cannot pinch it | Yes. It is the fat you can physically pinch |
| Metabolic Activity | Highly active. Releases inflammatory cytokines and free fatty acids | Relatively inactive. Acts primarily as energy storage |
| Effect on Insulin | Directly impairs insulin signalling and liver function via the portal vein | Minimal direct effect on insulin sensitivity |
| Disease Risk | Strongly associated with type 2 diabetes, cardiovascular disease, and metabolic syndrome | Generally neutral or protective, particularly in the lower body |
| Common Pattern | Apple shaped body. More common in men and post-menopausal women | Pear shaped body. More common in premenopausal women |
| Response to Exercise | Highly responsive. Preferentially reduced by aerobic and resistance training | Reduces more slowly and less preferentially than visceral fat |
Why Visceral Fat Drives Type 2 Diabetes
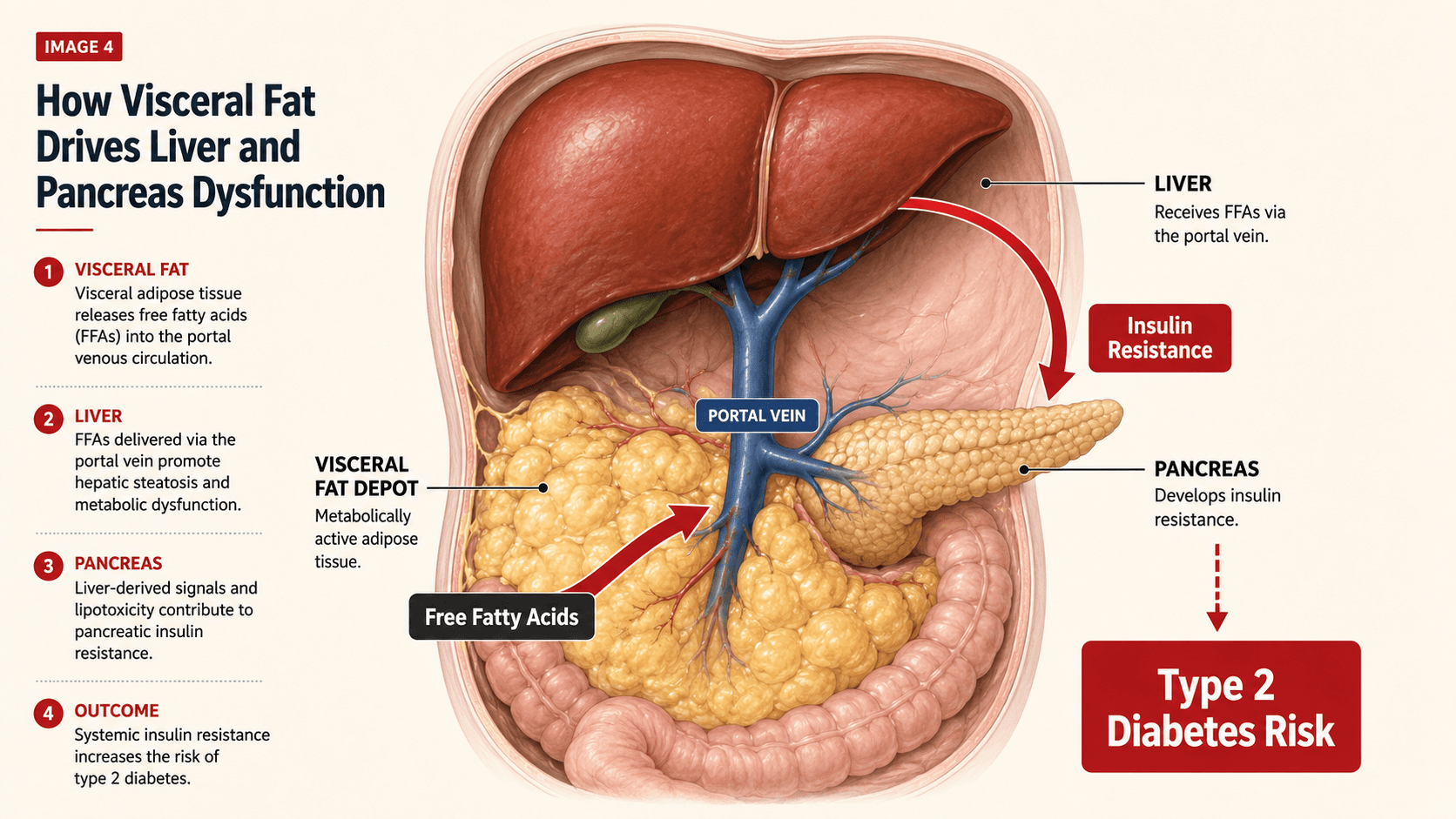
The relationship between visceral fat and type 2 diabetes is not simply a correlation. There is a clear mechanistic pathway that explains why carrying excess fat around your internal organs accelerates the progression from healthy metabolism to insulin resistance to full blown diabetes.
When visceral fat expands, it releases increasing quantities of free fatty acids directly into the portal circulation. These fatty acids reach the liver in high concentrations, where they impair the liver's ability to clear insulin from the bloodstream and reduce hepatic insulin sensitivity. The result is that more insulin is required to achieve the same blood glucose lowering effect. Over time, the pancreas has to work progressively harder, producing more and more insulin to compensate. This is insulin resistance, and it is the precursor to type 2 diabetes (5).
Visceral fat also produces a range of pro-inflammatory molecules including tumour necrosis factor alpha (TNF-α) and interleukin 6 (IL-6). These cytokines create a state of chronic low grade inflammation throughout the body, which further disrupts insulin signalling pathways in muscle, liver, and adipose tissue (2). It is a vicious cycle. The more visceral fat you carry, the more inflammation you produce, the worse your insulin sensitivity becomes, and the more likely your body is to store even more fat viscerally rather than subcutaneously.
A study published in Diabetes found that distinct fat distribution patterns are independently associated with future type 2 diabetes risk. The researchers identified that individuals with a hepatic steatosis pattern, meaning high fat deposition in the liver, had a fourfold greater risk of developing type 2 diabetes compared to those with the lowest fat accumulation pattern (6). The study also confirmed that both visceral fat at baseline and increases in visceral fat over time were strongly linked to higher diabetes incidence. This is not about total body weight. It is about where the fat sits and what it does when it gets there.
Why BMI Does Not Tell the Full Story
Body mass index is the most widely used measure of body composition in clinical practice, but it is a deeply flawed tool when it comes to assessing metabolic risk. BMI divides your weight in kilograms by your height in metres squared. It tells you nothing about where your weight is distributed, how much of it is muscle versus fat, or how much visceral fat you are carrying. Two men at 90 kilograms and 180 centimetres tall have the same BMI regardless of whether one is lean and muscular with a flat stomach and the other is carrying 15 kilograms of abdominal fat around his organs.
Research from the EPIC Potsdam study demonstrated that individuals of normal weight but with a large waist circumference had a significantly elevated risk of developing type 2 diabetes, in some cases exceeding the risk of individuals who were classified as overweight by BMI but who had a smaller waist circumference (7). The study concluded that both BMI and waist circumference should be measured together, because waist circumference provides critical information about visceral fat accumulation that BMI completely misses.
This is why I always measure waist circumference alongside body weight with my clients. It is a simple, free, and highly informative marker of visceral fat and metabolic risk. A waist circumference of 94 cm or above in men and 80 cm or above in women is associated with increased metabolic risk. Above 102 cm in men and 88 cm in women, the risk is substantially elevated (8). These thresholds are not perfect and vary by ethnicity, but they provide a far better picture of health risk than stepping on a scale alone.
Waist Circumference and Metabolic Risk: A Quick Reference
| Risk Level | Men | Women |
|---|---|---|
| Lower Risk | Below 94 cm (37 inches) | Below 80 cm (31.5 inches) |
| Increased Risk | 94 to 102 cm (37 to 40 inches) | 80 to 88 cm (31.5 to 34.5 inches) |
| Substantially Elevated Risk | Above 102 cm (40 inches) | Above 88 cm (34.5 inches) |
These thresholds are based on guidelines from the World Health Organisation and the International Diabetes Federation (8). They apply to European populations. South Asian, East Asian, and other ethnic groups may carry higher metabolic risk at lower waist circumference thresholds and should apply more conservative cutoffs. If you are of South Asian descent, for example, a waist circumference above 90 cm in men is considered elevated risk. I always encourage my clients to know their waist measurement and to track it over time alongside their body weight.
Men and Women Store Fat Differently and It Matters
There are significant sex based differences in fat storage patterns, driven primarily by hormones. Premenopausal women tend to store fat preferentially in subcutaneous depots in the hips, thighs, and buttocks. This is driven by oestrogen, which promotes subcutaneous fat deposition and protects against visceral accumulation. This is one of the reasons premenopausal women are at lower risk of type 2 diabetes and cardiovascular disease compared to men of the same age and body fat percentage (3).
Men, on the other hand, are more likely to store fat viscerally from the outset. Testosterone does not offer the same protective redistribution that oestrogen provides. This is why men tend to develop the classic beer belly or pot belly pattern while women of the same age tend to carry their weight lower on the body. It is also why men develop type 2 diabetes at a lower BMI than women on average.
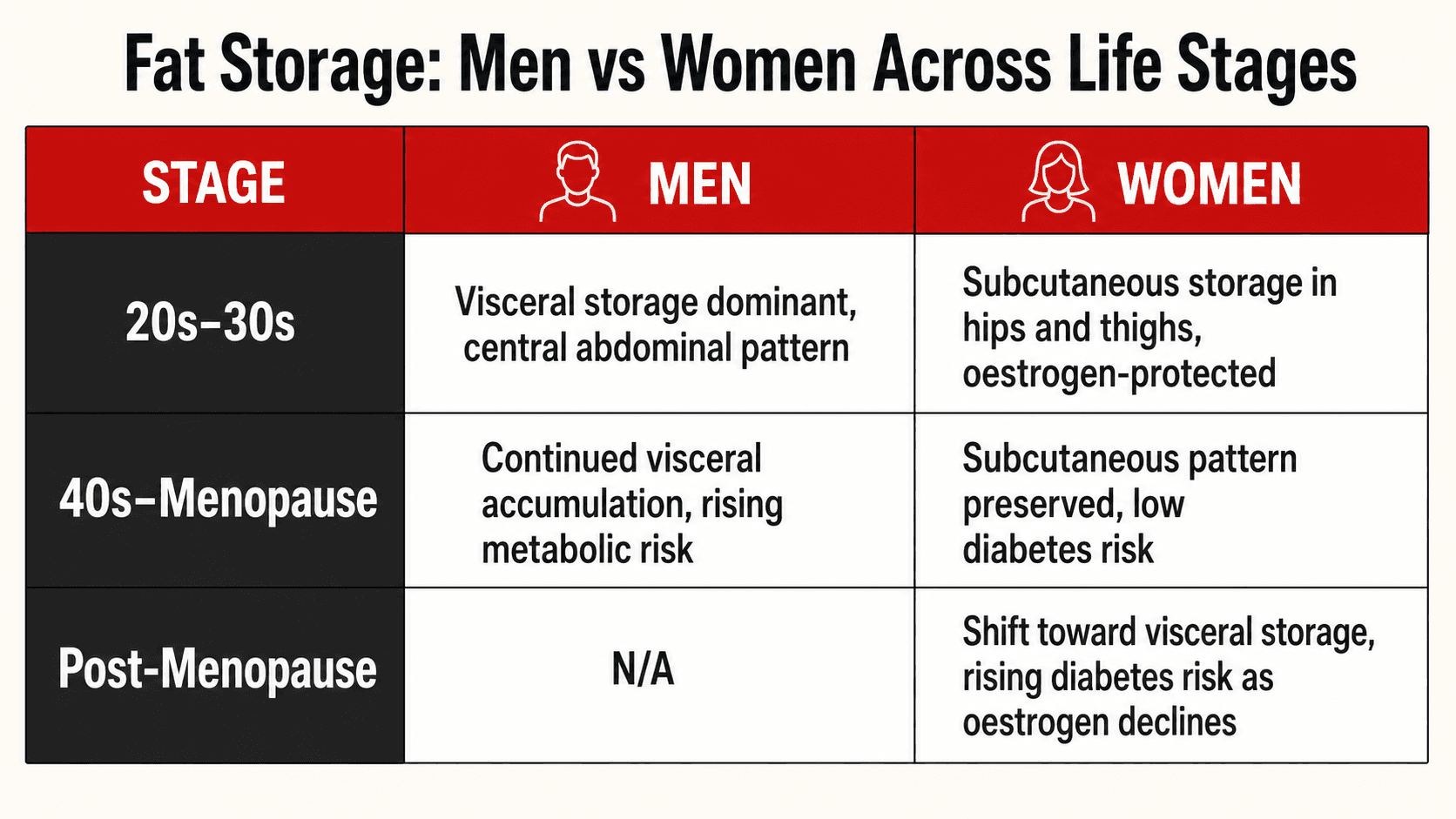
The picture changes significantly for women after menopause. As oestrogen levels decline, fat distribution shifts away from the lower body and towards the abdomen. Post-menopausal women begin to accumulate more visceral fat, and their risk of type 2 diabetes, metabolic syndrome, and cardiovascular disease rises accordingly (3). This is one of the reasons I pay close attention to body composition, waist circumference, and metabolic markers when working with female clients over 45. The protective hormonal environment they relied on for decades is changing, and their nutrition and training strategies need to adapt to reflect that.
Thin on the Outside, Fat on the Inside: The TOFI Phenomenon
One of the most dangerous misconceptions in health and fitness is that being slim means being healthy. There is a well documented phenomenon known as TOFI, which stands for thin on the outside, fat on the inside. These are individuals who appear lean and may have a normal BMI, but who carry disproportionately high levels of visceral fat and ectopic fat deposits in the liver, pancreas, and muscles. They are metabolically obese but visually lean.
Research has shown that approximately 10 to 20 percent of diabetes cases worldwide occur in individuals who are not classified as obese by BMI, and in some Asian countries this proportion rises to as high as 60 to 80 percent (9). This is a staggering figure. It means that millions of people who look and feel fine are walking around with dangerously dysfunctional metabolic profiles because their visceral fat levels are elevated even though their overall body mass is not.
This is exactly why I am always telling my clients that the number on the scale is only part of the picture. If you are slim but sedentary, if you eat poorly but stay thin, if you have never lifted a weight in your life but assume you are healthy because you fit into a size medium, you could be a TOFI. Waist circumference, fasting blood glucose, HbA1c, fasting insulin, and a lipid panel will tell you far more about your health than your body weight ever will.

How to Reduce Visceral Fat and Lower Your Diabetes Risk
The good news is that visceral fat is highly responsive to intervention. In fact, it is one of the first fat depots to reduce when you make the right changes to your nutrition, training, and lifestyle. A meta-analysis of 40 randomised controlled trials published in the British Journal of Sports Medicine found that both exercise and caloric restriction significantly reduced visceral fat, and that exercise demonstrated a clear dose-response relationship, meaning the more energy expended, the greater the reduction in visceral fat (10). Here is what the evidence supports.
Create a Sustained Calorie Deficit
Fat loss requires an energy deficit. There is no way around this fundamental principle. But the encouraging finding from the research is that visceral fat is preferentially mobilised during a calorie deficit, meaning it tends to reduce faster than subcutaneous fat when you are consistently in a deficit. You do not need an extreme approach. A moderate deficit of 400 to 600 calories per day, sustained over weeks and months, will drive meaningful reductions in visceral fat and significantly improve insulin sensitivity.
Prioritise Resistance Training
Resistance training builds and preserves lean muscle mass, which is critical for glucose disposal and metabolic health. A network meta-analysis of 84 randomised controlled trials found that aerobic exercise, resistance training, combined training, and high intensity interval training all significantly reduced visceral fat in overweight and obese individuals (11). Resistance training should form the backbone of any body composition programme. It improves insulin sensitivity independently of fat loss, it supports metabolic rate, and it gives your body somewhere useful to direct the glucose and amino acids from your food.
Add Aerobic Activity and Increase Your Daily Step Count
Aerobic exercise, even at moderate intensity, has a well established effect on visceral fat reduction. But you do not need to spend hours on a treadmill. Walking is one of the most effective and sustainable tools for increasing energy expenditure and reducing abdominal fat. Aim for a minimum of 8,000 to 10,000 steps per day and combine this with 2 to 4 structured training sessions per week.
Focus on Protein Intake
Adequate protein intake supports muscle retention during a fat loss phase, improves satiety, and has a higher thermic effect than carbohydrates or fat. I typically set my clients at 1.6 to 2.2 grams of protein per kilogram of body weight per day during a fat loss phase. For vegetarian and vegan clients, this means building meals around tofu, tempeh, seitan, lentils, chickpeas, soy protein, pea protein, and dairy or dairy alternatives depending on their dietary choices.
Prioritise Sleep and Manage Stress
Chronic sleep deprivation and elevated cortisol levels are both independently associated with increased visceral fat accumulation. Cortisol, the primary stress hormone, promotes the deposition of fat in visceral depots specifically. If you are training hard and eating well but sleeping five hours a night and running on chronic stress, you are fighting against your own biology. Seven to nine hours of quality sleep per night and deliberate stress management are non-negotiable components of any serious fat loss and health improvement plan.
Choose Lower Glycemic, Fibre Rich Carbohydrate Sources
Diets high in refined carbohydrates and added sugars promote visceral fat accumulation and worsen insulin resistance. Swapping refined carbohydrates for whole grains, legumes, vegetables, and lower glycemic options supports better blood sugar regulation and reduces the metabolic drivers of visceral fat storage. Oats, sweet potatoes, lentils, chickpeas, quinoa, and basmati rice are staples I use across my clients' meal plans regardless of whether they eat meat, are vegetarian, or are fully plant based.
Your Visceral Fat Reduction Checklist
| Strategy | Why It Works | Practical Target |
|---|---|---|
| Calorie Deficit | Visceral fat is preferentially mobilised during sustained energy deficit | 400 to 600 kcal deficit per day |
| Resistance Training | Builds muscle, improves insulin sensitivity, supports metabolic rate | 2 to 4 sessions per week |
| Aerobic Activity | Dose-dependent reduction in visceral fat with increasing energy expenditure | 150+ minutes moderate intensity per week |
| Daily Steps | Increases total energy expenditure without added fatigue or recovery cost | 8,000 to 10,000 steps per day |
| Protein Intake | Preserves lean mass, improves satiety, higher thermic effect | 1.6 to 2.2 g per kg body weight per day |
| Sleep | Poor sleep raises cortisol which promotes visceral fat deposition | 7 to 9 hours per night |
| Stress Management | Chronic cortisol elevation drives visceral fat storage specifically | Daily deliberate practice |
| Lower GI Carbohydrates | Reduces blood sugar spikes, improves insulin sensitivity, reduces visceral fat drivers | Prioritise whole grains, legumes, vegetables |
The Bottom Line
Where you store your body fat matters as much as how much you carry. Visceral fat, the fat stored deep inside your abdominal cavity around your organs, is the single most important fat depot when it comes to your risk of developing type 2 diabetes, insulin resistance, and metabolic disease. It is metabolically active, it drives inflammation, it impairs liver function, and it disrupts insulin signalling in ways that subcutaneous fat simply does not. BMI alone will not tell you whether you are at risk. Your waist circumference, your blood work, and your body composition paint a far more accurate picture.
The encouraging reality is that visceral fat is highly responsive to the right interventions. A structured calorie deficit, consistent resistance training, adequate protein, sufficient sleep, managed stress, and smart carbohydrate choices will reduce visceral fat faster than any other fat depot in your body. You do not need a complicated protocol. You need consistency, accountability, and a plan built around your individual needs.
If you want a personalised plan that addresses your body composition, your metabolic health, your dietary preferences, and your specific risk factors, get in touch through trperformancecoaching.com. I work one-to-one with clients online globally. Whether you eat meat, are vegetarian, vegan, or somewhere in between, whether you are managing diabetes, PCOS, hypertension, or simply want to lose fat and protect your long term health, I will build a programme that works for your body and your life.
Work with Me
Get a personalised coaching plan built around your goals, your schedule, and your life.
Enquire NowReferences
- Porter SA, Massaro JM, Hoffmann U, Vasan RS, O'Donnell CJ, Fox CS. Abdominal subcutaneous adipose tissue: a protective fat depot? Diabetes Care. 2009; 32(6): 1068-1075.
- Tchernof A, Després JP. Pathophysiology of human visceral obesity: an update. Physiological Reviews. 2013; 93(1): 359-404.
- Palmer BF, Clegg DJ. The sexual dimorphism of obesity. Molecular and Cellular Endocrinology. 2015; 402: 113-119.
- Stefan N. Causes, consequences, and treatment of metabolically unhealthy fat distribution. The Lancet Diabetes and Endocrinology. 2020; 8(8): 616-627.
- Neeland IJ, Ross R, Després JP, et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: a position statement. The Lancet Diabetes and Endocrinology. 2019; 7(9): 715-725.
- Yamazaki H, Tauchi S, Machann J, et al. Fat distribution patterns and future type 2 diabetes. Diabetes. 2022; 71(9): 1937-1945.
- Schulze MB, Heidemann C, Schienkiewitz A, Bergmann MM, Hoffmann K, Boeing H. Body mass index, waist circumference, and the risk of type 2 diabetes mellitus: implications for routine clinical practice. Deutsches Ärzteblatt International. 2010; 107(26): 470-476.
- Klein S, Allison DB, Heymsfield SB, et al. Waist circumference and cardiometabolic risk: a consensus statement from Shaping America's Health. Diabetes Care. 2007; 30(6): 1647-1652.
- Gujral UP, Weber MB, Staimez LR, Narayan KMV. Diabetes among non-overweight individuals: an emerging public health challenge. Current Diabetes Reports. 2018; 18(8): 60.
- Verheggen RJHM, Maessen MFH, de Groot DRMJ, Hermus ARMM, Eijsvogels TMH, Hopman MTE. Dose-response effects of exercise and caloric restriction on visceral adiposity in overweight and obese adults: a systematic review and meta-analysis of randomised controlled trials. British Journal of Sports Medicine. 2023; 57(16): 1035-1041.
- Chen N, Guo J, Xiang T, et al. Effects of various exercise types on visceral adipose tissue in individuals with overweight and obesity: a systematic review and network meta-analysis of 84 randomized controlled trials. Obesity Reviews. 2024; 25(2): e13666.
