The Belief That Is Doing More Damage Than Any Programme Failure
Neuroplasticity is the scientific term for the brain's capacity to change its own structure and function in response to experience, learning, and behaviour. It is one of the most important findings in modern neuroscience, and its implications for anyone who has ever told themselves they are too old to change, too set in their ways to build new habits, or simply not the kind of person whose brain works that way, are profound and genuinely life-changing when properly understood.
The belief that the adult brain is fixed, that its fundamental architecture is established in childhood and adolescence and thereafter immutable, was the dominant scientific consensus until the latter decades of the twentieth century. The practical consequence of this belief in health behaviour is widespread and damaging. It is the sentence structure behind every I am too old to change now, every my metabolism is just like this, every I have always been someone who, and every I cannot teach an old dog new tricks that has ever been deployed in defence of an unchanged health behaviour in a person who genuinely wanted to change it.
That belief is wrong. Not aspirationally wrong in the way that motivational content often overstates its case. Factually wrong, in the sense of being contradicted by decades of peer-reviewed neuroscience that has established with considerable precision both the mechanisms by which the adult brain changes its own structure and function in response to experience, and the conditions under which those changes are most and least likely to occur. The age at which neuroplasticity ceases to be available is, for all practical purposes of health behaviour change, not reached within a normal human lifespan.
“The brain is not a static organ. It changes with every thought, memory, and experience. The question is never whether it can change. It is always whether you are giving it the experiences it needs to change in the direction you want.”
— Michael Merzenich
Hebb's Rule and the Mechanism of Neural Change: How Repetition Rewires the Brain
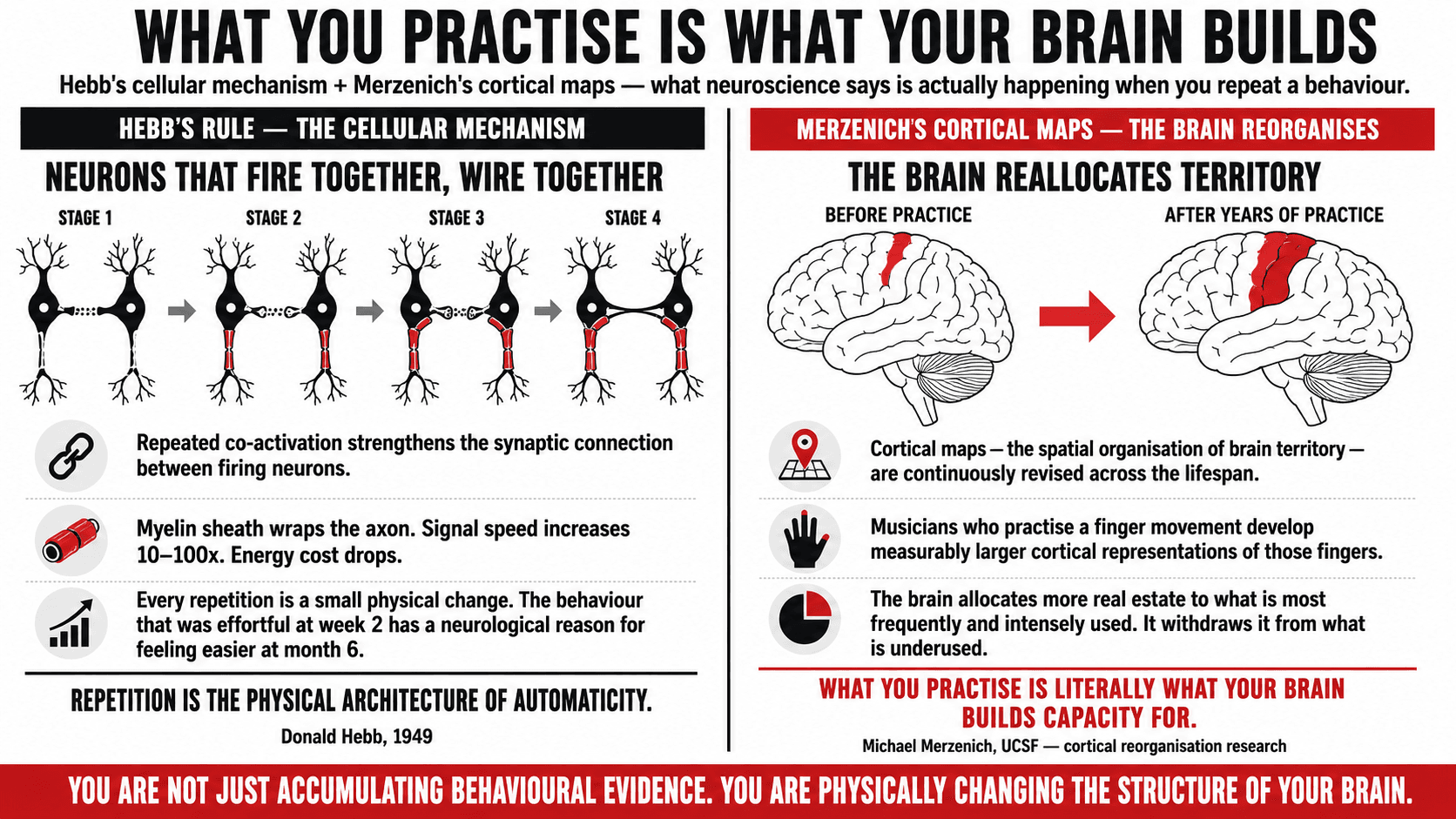
The foundational principle of neuroplasticity was articulated by the Canadian neuroscientist Donald Hebb in 1949, in a formulation so precise and so enduring that it is still the mechanistic foundation of the field more than seventy years later. Hebb's rule, colloquially summarised as neurons that fire together wire together, describes the cellular mechanism by which repeated co-activation of neural pathways produces a strengthening of the synaptic connections between them. Each time a behaviour is performed, a set of neurons fires in a particular sequence. The firing of this sequence, if it is repeated, produces structural changes at the synaptic connections between the neurons involved: the connections become stronger, faster, and more reliable. The pathway becomes more automatic with each repetition (1).
The physical substrate of this process is myelination: the wrapping of the axons of active neurons in a sheath of myelin, a fatty insulating material produced by glial cells called oligodendrocytes. Myelination increases the speed and reliability of neural signal transmission along the pathway by a factor of between ten and one hundred, depending on the degree of myelination. A well-myelinated neural pathway is a fast, reliable, low-energy pathway. It is the neural architecture of automaticity: the behaviour that was once effortful and deliberate has become, through repetition-driven myelination, the behaviour that requires minimal conscious attention and feels, from the inside, completely natural.
Michael Merzenich, widely considered the world's leading authority on adult neuroplasticity, extended Hebb's cellular observations into the domain of brain organisation, demonstrating through decades of research that the brain's cortical maps, the spatial organisation of neural territory allocated to different functions, are continuously revised throughout the lifespan in response to the patterns of experience the brain is receiving. Merzenich's research showed that musicians who practise a particular finger movement over years develop measurably larger cortical representations of the fingers involved. The brain allocates more neural real estate to the functions that are most frequently and intensely used, and withdraws it from functions that are underused. The implication is direct: what you practise consistently is what your brain builds capacity for, regardless of age (2).
Norman Doidge's documentation of neuroplasticity case studies in The Brain That Changes Itself brought these laboratory findings into vivid clinical relief, describing individuals who had recovered motor function after strokes, rebuilt language capacity after brain injury, and fundamentally altered the organisation of their sensory processing through targeted behavioural practice. The central message across all of these cases, which Doidge was careful to ground in the mechanistic neuroscience of Merzenich and others, is that the brain responds to experience at any age. The rate of response varies. The ease of change varies. The capacity for it does not cease (3).
Key Insight: Every time you complete a training session, eat a meal that serves your health, or maintain a healthy behaviour under pressure, you are not just accumulating behavioural evidence for the identity you are building. You are physically changing the structure of your brain. The myelin sheath thickens with each repetition. The pathway becomes faster and more reliable. What feels effortful and deliberate at week two has a neurological reason for feeling easier at month six. You are not simply getting used to it. You are literally rewiring.
The Neural Pathway Myelination Progression: What Is Happening in Your Brain Across the Stages of a New Habit
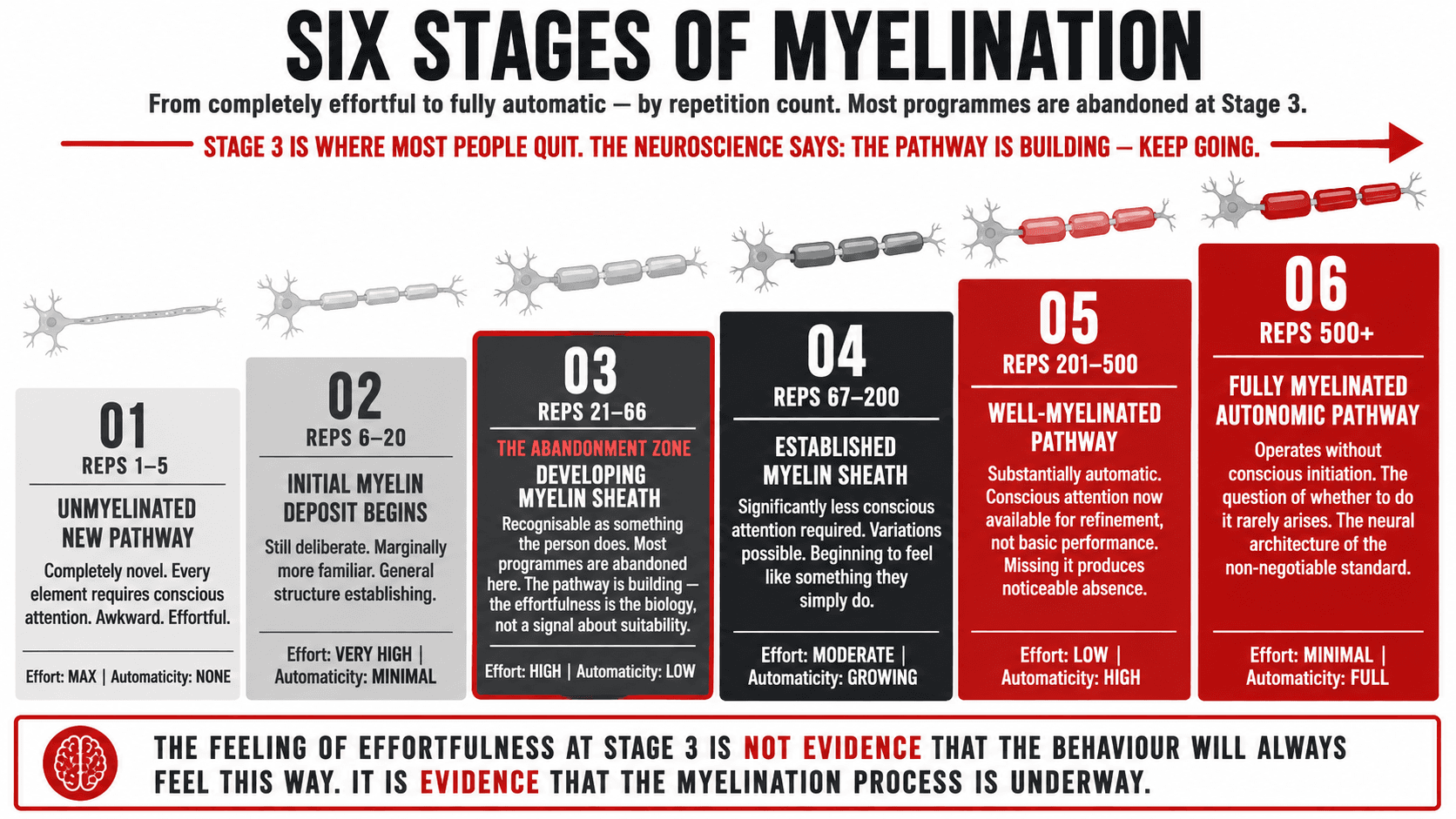
The process of myelination is not a binary event. It is a continuous progression from the thin, slow, unreliable neural pathway of a new behaviour to the thick, fast, automatic pathway of an established habit. The table below maps this progression across six stages, from the first encounter with a new behaviour through to full automaticity, showing what is happening neurologically at each stage, what the behaviour feels like from the inside, and the approximate repetition count at which each stage is typically reached in a healthy adult.
These are approximate ranges based on current neuroscience. The actual rate of progression varies significantly with sleep quality, the emotional significance of the behaviour, the degree of focused attention brought to the practice, and the individual's baseline neurological health. All of these factors can be influenced, which means the rate of neuroplastic change is not fixed even if the mechanism itself is.
| Stage | Repetitions (approx.) | Pathway State | What the behaviour feels like | Effort Required | Automaticity |
|---|---|---|---|---|---|
| 1 | 1 to 5 | Unmyelinated new pathway | Completely novel. Every element requires conscious attention. The behaviour feels awkward, unnatural, and effortful. Mistakes are common. Uncertainty about whether it is being done correctly. | Maximum | None |
| 2 | 6 to 20 | Initial myelin deposit begins | Still deliberate but marginally more familiar. Some elements are beginning to require less conscious oversight. The general structure of the behaviour is establishing. Still feels effortful and unnatural. | Very High | Minimal |
| 3 | 21 to 66 | Developing myelin sheath | The behaviour is becoming recognisable as something the person does. Elements of it are beginning to feel familiar if not yet natural. This is the stage most commonly described as the 21-day habit formation period, though actual myelination continues well beyond it. | High | Low |
| 4 | 67 to 200 | Established myelin sheath | The behaviour now requires significantly less conscious attention for its basic execution. Variations and refinements are possible. The person can think about something else during parts of the behaviour. It is beginning to feel like something they simply do. | Moderate | Growing |
| 5 | 201 to 500 | Well-myelinated pathway | The behaviour is substantially automatic for its standard execution. Conscious attention is available for refinement and quality rather than basic performance. Missing the behaviour now produces a noticeable absence rather than relief. | Low | High |
| 6 | 500+ | Fully myelinated autonomic pathway | The behaviour operates without conscious initiation for its standard execution. The question of whether to perform it rarely arises because it has moved into the category of things that simply happen as part of how the day is structured. This is the neural architecture of the non-negotiable standard. | Minimal | Full |
The most important point in this progression is Stage 3: the 66 to 200 repetition window where the behaviour is becoming established but is not yet reliably automatic. This is the stage at which most programmes are abandoned, and at which most people conclude that the behaviour is not working or not for them. The neuroscience says otherwise. The pathway is building. The automaticity is coming. The feeling of effortfulness at Stage 3 is not evidence that the behaviour will always feel this way. It is evidence that the myelination process is underway.
Why Sleep Is the Most Underrated Tool for Accelerating Neuroplastic Change
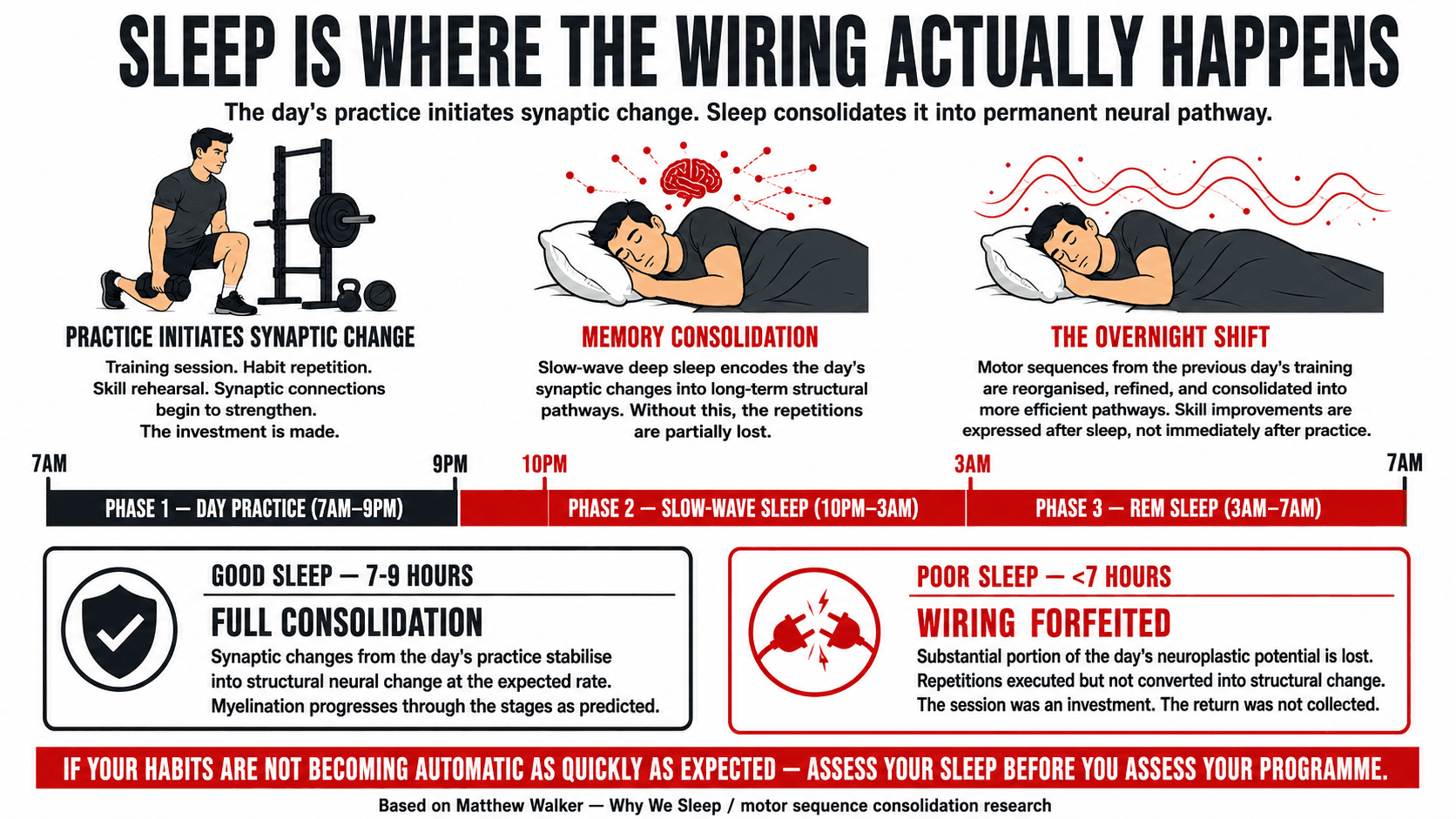
The relationship between sleep and neuroplasticity is one of the most practically significant findings in modern neuroscience, and one that is almost entirely absent from mainstream health and fitness conversation about habit formation. Memory consolidation, the process by which the experiences and learning of the day are encoded into long-term structural changes in the brain, occurs primarily during slow-wave sleep and REM sleep. The synaptic changes initiated by the day's learning and practice are stabilised and integrated during sleep. Without adequate sleep, the neuroplastic changes initiated by practice are partially or substantially lost, and the repetition that should have advanced the myelination process fails to produce its full structural benefit (4).
The practical implication is direct: the person who trains consistently but sleeps poorly is performing a significant volume of repetitions that are not being fully converted into neural pathway development at the rate they should be. The myelination progression table above assumes adequate sleep. Under conditions of chronic sleep deprivation, which Matthew Walker defines as fewer than seven hours for adults, the progression is materially slower. The person who wonders why their habits are not becoming automatic as quickly as expected despite consistent practice should consider sleep quality as seriously as they consider training quality. The two are not separate variables in the neuroplasticity equation.
Sleep also has a specific role in motor skill consolidation, the category of learning most relevant to physical training. Research on motor sequence learning shows that the performance improvements from a practice session are substantially expressed not immediately after practice but following the subsequent night of sleep, a phenomenon Walker describes as the overnight shift. The sleep period following a training session is not merely a recovery window. It is an active neurological processing period during which the motor sequences practised during the session are reorganised, refined, and consolidated into more efficient neural pathways. Skipping the sleep does not just impair recovery. It forfeits a substantial portion of the adaptation that the session was designed to produce (5).
Key Insight: If you are training consistently and finding that the behaviours are not becoming automatic as quickly as you expected, assess your sleep before you assess your programme. Seven to nine hours of quality sleep per night is not a luxury that supports neuroplastic change. It is the mechanism through which practice becomes wiring. Without it, repetition produces less than half the structural benefit it should. The session is an investment. The sleep is where the return is collected.
Age and Neuroplasticity: What Changes, What Does Not, and Why It Matters Less Than You Think
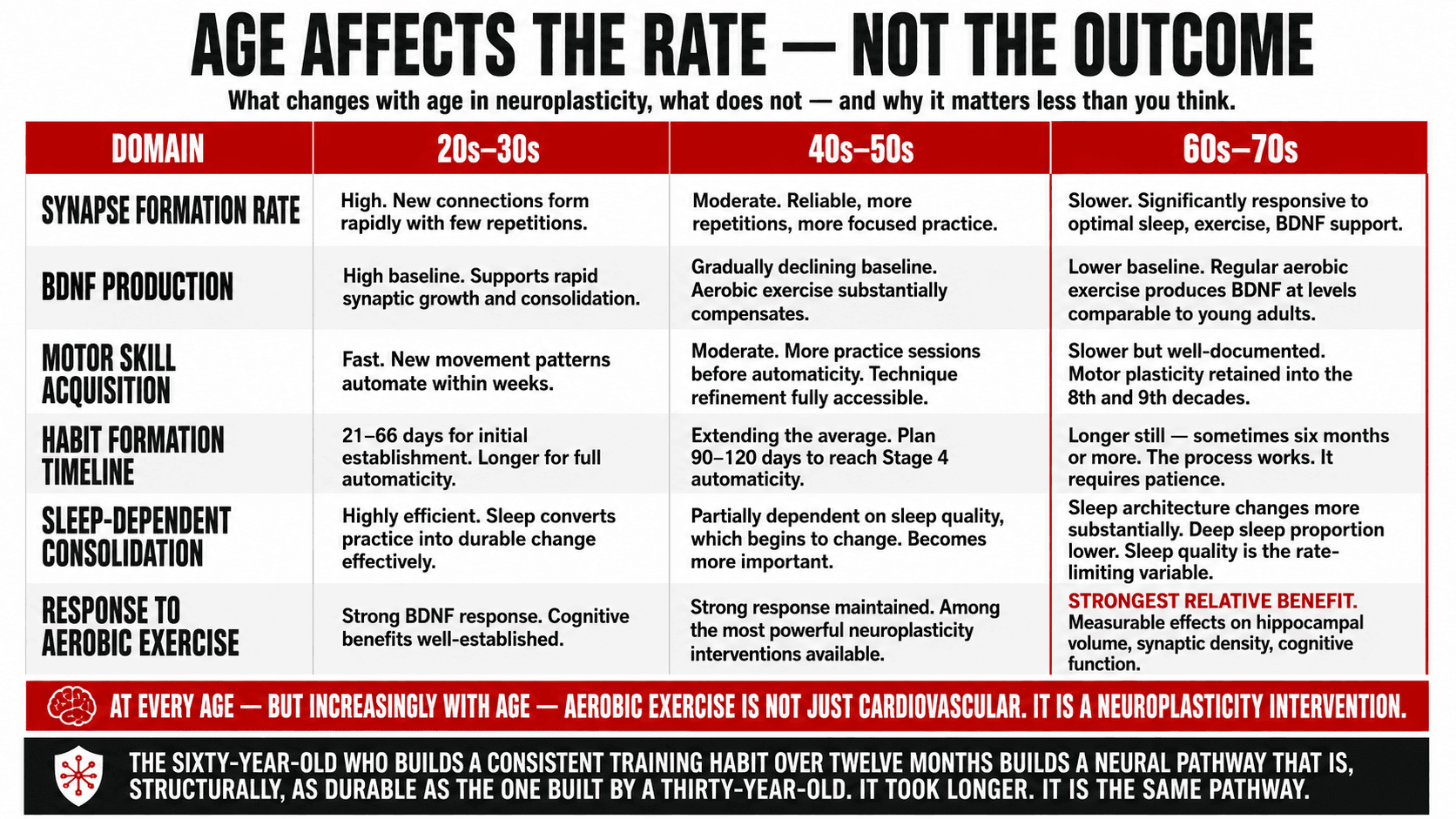
The honest account of age and neuroplasticity requires acknowledging both what the research shows does change with age and what it shows remains available throughout the lifespan. The brain does change with age in ways that are relevant to the rate and ease of neuroplastic change. The rate of new synapse formation slows somewhat in middle age compared to childhood. The production of BDNF, brain-derived neurotrophic factor, the protein most closely associated with synaptic growth and plasticity, declines gradually from the mid-twenties onward. The myelination progression described above takes longer in a person of fifty than in a person of twenty-five. These are real differences that honest neuroscience does not deny (6).
What the same research consistently shows, and what is far more important for the purposes of health behaviour change, is that these differences affect rate rather than capacity. The adult brain retains the full neuroplastic mechanism throughout the lifespan. The same cellular processes that produce habit formation in a twenty-five year old produce habit formation in a sixty year old. The sixty year old typically requires more repetitions to reach the same level of automaticity and benefits more from optimal sleep, stress management, and physical exercise as supporting conditions for neuroplasticity. But the destination is available. The neuroplastic change that produces a new automatic healthy behaviour is not conditional on age.
| Neuroplasticity Domain | 20s to 30s | 40s to 50s | 60s to 70s | Practical Implication |
|---|---|---|---|---|
| Synapse formation rate | High. New synaptic connections form rapidly with relatively few repetitions. | Moderate. New connections form reliably but require more repetitions and benefit from more focused practice. | Slower. New connections form at reduced rate. Benefits significantly from optimal sleep, aerobic exercise, and BDNF-supporting behaviours. | Older adults need more repetitions to reach automaticity but do reach it. The trajectory is the same. The timeline is longer. |
| BDNF production | High baseline. BDNF levels support rapid synaptic growth and efficient consolidation. | Gradually declining baseline. BDNF is responsive to aerobic exercise, which can substantially compensate for age-related decline. | Lower baseline. Aerobic exercise, particularly zone two steady-state cardio, produces BDNF at levels comparable to those achieved in younger adults following regular training. | This is the most actionable variable in age-related neuroplasticity. Regular aerobic exercise measurably increases BDNF production at any age. Fitness is a neuroplasticity intervention. |
| Motor skill acquisition | Fast. New movement patterns acquire automaticity within weeks with consistent practice. | Moderate. New movement patterns require more practice sessions before automaticity is established. Technique refinement is accessible throughout this decade. | Slower, but well-documented in research. Motor plasticity is retained into the eighth and ninth decades. Learning new movement patterns in the sixties and seventies is well-supported by the literature. | The person who believes they are too old to learn new movement patterns, new training techniques, or new physical skills is working from outdated neuroscience. The capacity exists at all ages studied. |
| Habit formation timeline | Variable. Research suggests 21 to 66 days for initial establishment, longer for full automaticity. | Variable and generally longer. The 66-day average extends. Planning for 90 to 120 days to reach Stage 4 automaticity is realistic. | Longer again, with high individual variation. Some habits establish quickly, others require sustained repetition over six months or more. The process works. It simply requires patience. | The single most important adjustment for older adults building new health habits is patience with the timeline. The neuroplastic mechanism is working. The myelination is occurring. It is occurring more slowly. That is a timeline adjustment, not a capacity limitation. |
| Sleep-dependent consolidation | Highly efficient. Sleep converts practice into durable neural change effectively. | Partially dependent on sleep quality, which begins to change in middle age. Deep sleep proportion declines somewhat. Supporting sleep quality becomes more important. | Sleep architecture changes more substantially. Deep sleep proportion lower. The sleep-neuroplasticity relationship remains but requires more deliberate support of sleep quality. | At every age, but increasingly with age, sleep quality is the rate-limiting variable in neuroplastic change. This is within the person's control and should be treated as a primary training variable. |
| Response to aerobic exercise | Strong BDNF response to aerobic exercise. Cognitive benefits well-established. | Strong response maintained. Regular aerobic exercise at this age is one of the most powerful neuroplasticity interventions available, producing BDNF that partially offsets age-related decline. | Strongest relative benefit. Aerobic exercise in the sixties and seventies produces BDNF increases that have measurable effects on hippocampal volume, synaptic density, and cognitive function. | For older adults specifically, aerobic exercise is not just a cardiovascular and metabolic intervention. It is a neuroplasticity intervention. Zone two steady-state cardio three to four times per week supports the brain's capacity for the other changes on this list. |
The consistent finding across all age-related neuroplasticity research is that the variables most associated with slower change in older adults, BDNF production, sleep quality, and baseline aerobic fitness, are all substantially modifiable through behaviour. The person who trains aerobically, sleeps well, and manages stress is operating their neuroplasticity at a level that the chronological age alone does not predict.
The Fixed Mindset as a Self-Fulfilling Neurological Prophecy
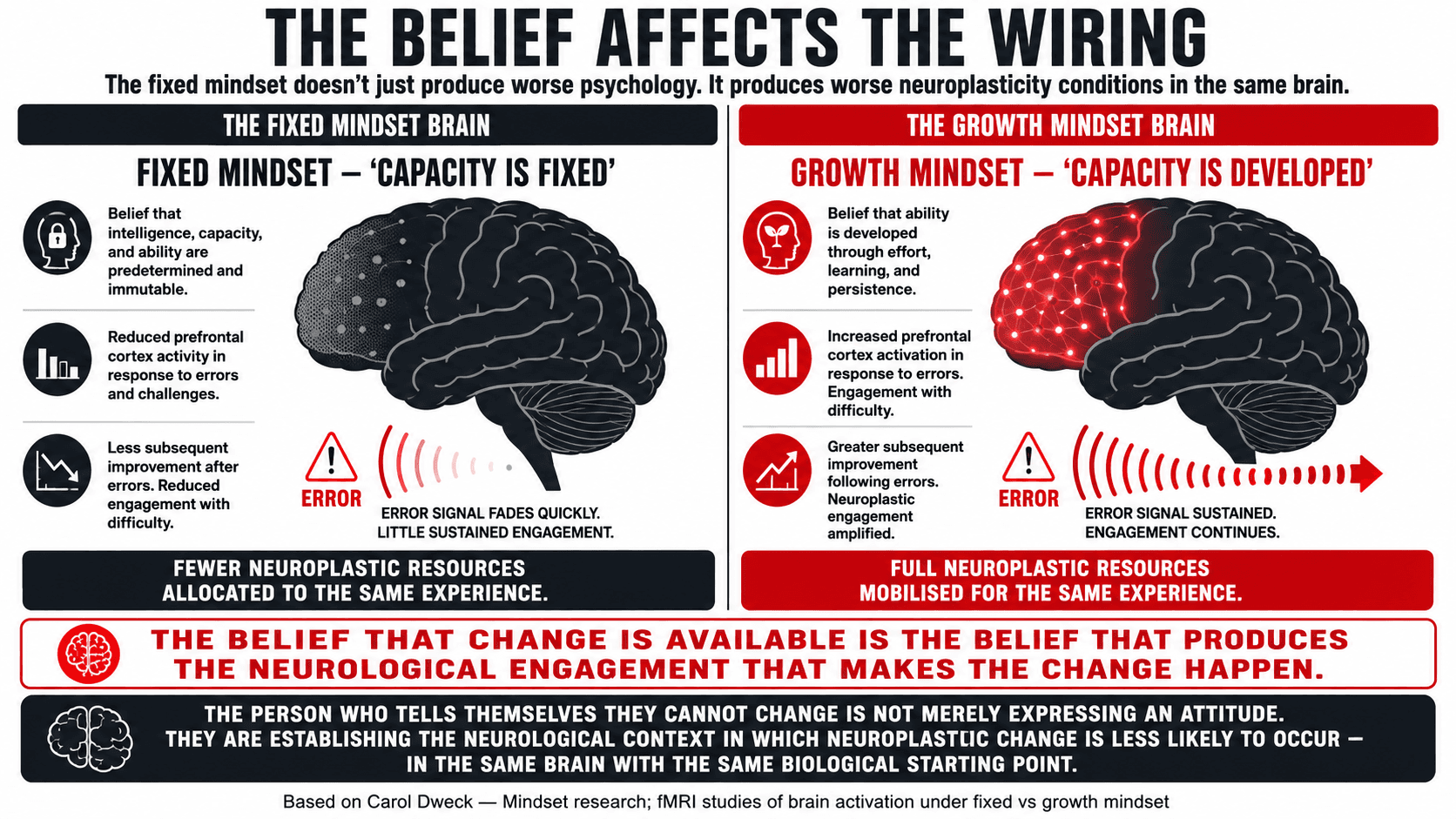
Carol Dweck's fixed versus growth mindset research takes on a specific additional significance in the context of neuroplasticity. The fixed mindset, the belief that intelligence, capacity, and ability are predetermined and immutable, does not merely produce worse psychological responses to setback and challenge. It also produces neurological conditions that make the neuroplastic change it denies less likely to occur. Dweck's research shows that people with fixed mindsets show different brain activation patterns in response to errors and challenges: reduced activity in the prefrontal cortex regions associated with engagement with difficulty, and less subsequent improvement in performance following errors, compared to individuals with growth mindsets (7).
The person who tells themselves they cannot change is not just expressing a psychological attitude. They are establishing a neurological context in which the conditions for neuroplastic change are less optimal than they would be in the same person with the same biological starting point and a different belief. The belief that change is available and that effort produces development activates the neural engagement with challenge that produces the neuroplastic response. The belief that capacity is fixed reduces that engagement and therefore reduces the neuroplastic response to the same experience. The mindset is not just a frame. It is a variable in the neuroplasticity equation.
This is one of the reasons why the identity work, establishing the identity of the person you are becoming before the evidence for that identity exists in full, is not merely motivational scaffolding. It is establishing the psychological and neurological conditions under which the neuroplastic change that will eventually make the behaviour automatic is most likely and most rapid. The growth mindset that believes the change is available is the mindset that produces the neurological engagement that makes the change happen.
Key Insight: The belief I cannot change that kind of behaviour is a statement about the past, not about the biology. Every piece of neuroscience in this article applies to you specifically, with your specific age, your specific history, and your specific starting point. The mechanism is universal. The rate varies. The outcome, with sufficient repetition and the right conditions, is available. The question is not whether your brain can build the pathway. It is whether you will give it the repetitions it needs to do so.
What the Trainable Brain Means for How You Approach the Programme
The practical implications of neuroplasticity for health behaviour are not complicated, but they require a reframing of some assumptions that are deeply embedded in the way most people think about habit formation and change. The most important reframe is the relationship between current difficulty and future automaticity. The fact that a behaviour is effortful, uncomfortable, and requiring deliberate attention right now is not evidence that it will always feel this way. It is evidence that the myelination process is at an early stage. The effort is the biology of early-stage neural pathway formation. It is not a signal about the person's suitability for the behaviour.
The second reframe is the relationship between age and capacity. Every person I have worked with who has said some version of I am too old to change fundamentally has been operating from a model of neuroplasticity that was superseded by the science decades ago. The rate of change is different at different ages. The capacity for it is not. The sixty-year-old who builds a consistent training habit over twelve months and maintains it for five years has built a neural pathway that is, by the end of that period, as automatic and as durable as the one built by a thirty-year-old. It took longer. It required more sleep, more patience, and probably more conscious attention in the early stages. The pathway is structurally the same.
I work with clients at every stage of life. I work with clients in their twenties who are building their first serious relationship with training and nutrition. I work with clients in their fifties and sixties who are rebuilding a relationship with their health that was allowed to deteriorate during a demanding professional period. The neuroscience does not distinguish between these cases in terms of the available outcome. It distinguishes them only in terms of the timeline and the conditions that support it most effectively. I work one-to-one online globally. The conversation about what is possible, neuroscience first, is where we begin.
Work with Me
Get a personalised coaching plan built around your goals, your schedule, and your life.
Enquire NowReferences
- Hebb DO. The Organisation of Behavior: A Neuropsychological Theory. New York: Wiley; 1949.
- Merzenich MM, Kaas JH, Wall J, et al. Topographic reorganization of somatosensory cortical areas 3b and 1 in adult monkeys following restricted deafferentation. Neuroscience. 1983; 8(1): 33-55.
- Doidge N. The Brain That Changes Itself: Stories of Personal Triumph from the Frontiers of Brain Science. New York: Viking; 2007.
- Stickgold R. Sleep-dependent memory consolidation. Nature. 2005; 437(7063): 1272-1278.
- Walker MP, Brakefield T, Morgan A, et al. Practice with sleep makes perfect: sleep-dependent motor skill learning. Neuron. 2002; 35(1): 205-211.
- Bherer L, Erickson KI, Liu-Ambrose T. A review of the effects of physical activity and exercise on cognitive and brain functions in older adults. Journal of Aging Research. 2013; 2013: 657508.
- Dweck CS. Mindset: The New Psychology of Success. New York: Random House; 2006.
- Cotman CW, Berchtold NC, Christie LA. Exercise builds brain health: key roles of growth factor cascades and inflammation. Trends in Neurosciences. 2007; 30(9): 464-472.