
Prostate health is the subject most men are least comfortable discussing and least informed about. It sits at an uncomfortable intersection of medical anxiety, masculinity, and bodily awareness that most men have never been encouraged to develop. The result is that the most common cancer in UK men is also one of the most poorly understood, most inconsistently screened for, and most frequently detected too late.
This article will not alarm you unnecessarily. It will give you a clear, evidence-based understanding of what the prostate is, what can go wrong with it, what your risk profile looks like, and what you can do through lifestyle to meaningfully reduce that risk. It will also tell you exactly what to say to your GP and when to say it.
Knowledge is not anxiety. It is the precondition for action.
The Gland Most Men Never Think About Until Something Goes Wrong
Prostate cancer will be diagnosed in approximately one in eight men in the UK during their lifetime. It is the most common cancer in men, accounting for around 26 percent of all male cancer diagnoses. Each year, roughly 52,000 men in the UK are diagnosed and around 12,000 die from it — a mortality figure that is largely a consequence of late detection rather than an inevitable feature of the disease.
The uncomfortable truth is that most men arrive at a prostate cancer diagnosis having never considered the possibility, having never discussed it with a doctor proactively, and having never made any of the lifestyle modifications that could have reduced their risk or improved their prognosis.
This is not a failure of intelligence. It is a failure of education and a consequence of a culture in which men are not taught to engage with their health until something goes wrong. That culture costs lives.
What the Prostate Is and What It Actually Does
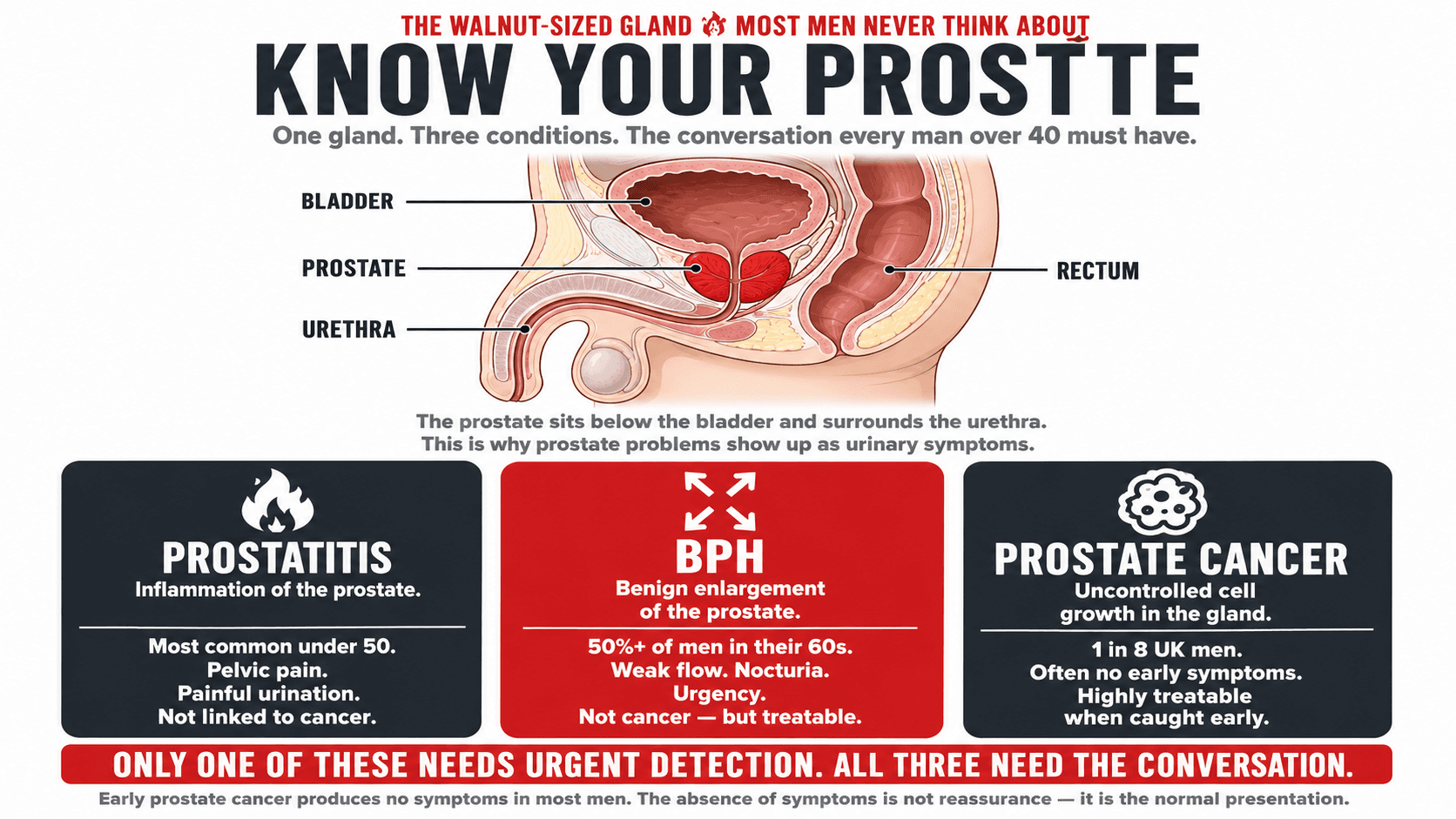
The prostate is a walnut-sized gland located just below the bladder and in front of the rectum. It surrounds the urethra — the tube that carries urine and semen out of the body — which is why prostate problems so often manifest as urinary symptoms. Its primary function is to produce prostatic fluid, a component of semen that nourishes and protects sperm during ejaculation.
The prostate is highly sensitive to hormonal signalling, particularly androgens such as testosterone and its more potent derivative dihydrotestosterone (DHT). This hormonal sensitivity underpins both its normal function and its susceptibility to certain disease processes. Prostate cancer cells, in particular, are often androgen-dependent in their early stages — meaning they require testosterone to grow — which is why androgen deprivation therapy is used as a treatment strategy in more advanced cases.
The prostate also undergoes natural growth throughout a man's life, which is why conditions such as benign prostatic hyperplasia become almost universal with advancing age.
Practical Takeaway
If you are a man over 40 and you have noticed any changes in urinary flow, increased frequency at night, difficulty starting or stopping urination, or a sensation of incomplete bladder emptying, these symptoms warrant a conversation with your GP. They may have a benign cause, but they should not be ignored or assumed to be insignificant.
Know Your Prostate: The Three Main Conditions
The three primary conditions affecting the prostate are distinct in their causes, symptoms, and management. Understanding the differences will help you engage more effectively with healthcare providers and reduce unnecessary anxiety when symptoms arise.
Prostatitis
Prostatitis refers to inflammation of the prostate and is the most common prostate condition in men under 50. It can be bacterial in origin (acute or chronic bacterial prostatitis) or non-bacterial (chronic pelvic pain syndrome), with the latter being far more common and less well understood. Symptoms include pelvic pain, painful urination, painful ejaculation, and in acute bacterial cases, fever and systemic illness. Prostatitis is not associated with an increased risk of prostate cancer but can significantly impair quality of life.
Benign Prostatic Hyperplasia (BPH)
BPH is a non-cancerous enlargement of the prostate. Histological evidence of BPH is present in over 50 percent of men in their 60s and over 80 percent of men in their 80s. Because the enlarged prostate presses against the urethra, BPH causes the urinary symptoms that many men assume are simply an inevitable part of ageing — weak urine flow, urgency, nocturia (waking at night to urinate), and incomplete bladder emptying. BPH does not become prostate cancer but shares some of the same hormonal drivers.
Prostate Cancer
Prostate cancer is the uncontrolled growth of cells within the prostate gland. It is often slow-growing and, when detected early, highly treatable. However, more aggressive forms exist and, when detected late, prostate cancer becomes substantially harder to treat effectively. Unlike BPH or prostatitis, early-stage prostate cancer often produces no symptoms at all — which is why proactive screening matters.
BPH: The Condition That Affects Most Men Over 50
BPH is so prevalent that it is tempting to frame it as an inevitable consequence of ageing. It is not. While age is the dominant risk factor and some degree of prostate growth is near-universal in older men, the severity of BPH symptoms and their functional impact are substantially modifiable.
Obesity and metabolic syndrome are strongly associated with more severe BPH symptoms. The mechanism is multifactorial: elevated oestrogen levels in men with excess body fat alter the hormonal environment of the prostate; chronic low-grade inflammation associated with visceral adiposity drives prostatic growth; and insulin resistance, which is almost universally present in overweight men, has independent effects on prostate cell proliferation.
Regular physical activity, particularly resistance training, is associated with reduced BPH symptom severity in multiple prospective studies. A 2008 analysis from the Health Professionals Follow-up Study found that men who exercised regularly were approximately 25 percent less likely to develop symptomatic BPH than sedentary men. The protective effect was seen across all forms of exercise but was most pronounced in vigorous activity.
Diet also plays a role. High intake of red meat and dietary fat has been positively associated with BPH progression, while vegetables — particularly those rich in lycopene and flavonoids — appear protective. Alcohol, particularly beer, has been associated with increased BPH risk, possibly through its effects on oestrogen metabolism.
Practical Takeaway
If you are experiencing urinary symptoms consistent with BPH, reducing central body fat through resistance training and nutrition is not just a cosmetic intervention — it is directly relevant to your prostate health. Men who improve their metabolic status often report meaningful reduction in urinary symptom severity. This does not replace medical evaluation, but it operates alongside it.
Prostate Cancer: The Facts Without the Fear
Prostate cancer has an unjustly frightening reputation given that, when detected early, it has a five-year survival rate of approximately 100 percent. The fear is not irrational — advanced prostate cancer is serious — but it is disproportionate to the actual prognosis in the majority of cases, which involve localised disease that is highly responsive to treatment.
The problem is not that prostate cancer is inherently unbeatable. The problem is that too many men are diagnosed too late because they never had the prostate conversation.
Early prostate cancer produces no symptoms in most men. The absence of symptoms is not reassurance. It is the normal presentation. A man can have significant localised prostate cancer with a completely normal urinary function. Symptoms tend to emerge only when the prostate has enlarged enough to affect the urethra or when cancer has spread to adjacent tissues. Waiting for symptoms before seeking evaluation is, in many cases, waiting too long.
Prostate cancer risk increases substantially with age. It is rare under 50, common in men in their 60s and 70s, and almost universal as a histological finding in men who live into their 80s and 90s (though most of these cancers are clinically insignificant). The critical distinction is between indolent prostate cancer — slow-growing tumours that may never cause harm during a man's lifetime — and aggressive prostate cancer, which requires prompt treatment.
This distinction is part of the reason prostate cancer screening remains more complex than screening for some other cancers. Detecting all prostate cancers is not the challenge. Distinguishing those that need treatment from those that can be safely monitored is the clinical task.
Practical Takeaway
If you are of Black African or Black Caribbean heritage, or if your father or brother has been diagnosed with prostate cancer, you are in a higher-risk group. The NHS currently recommends that men in these groups be made aware of their elevated risk and be offered a PSA test from age 45. Do not wait to be told you are high risk. If this applies to you, raise it proactively with your GP.
PSA Testing and Screening: What You Actually Need to Know
Prostate-Specific Antigen (PSA) is a protein produced by both normal and cancerous prostate cells. A blood test measuring PSA levels is currently the primary screening tool for prostate cancer in the UK, though it is not a definitive diagnostic test. Elevated PSA can be caused by prostate cancer, BPH, prostatitis, recent sexual activity, vigorous exercise, or urinary tract infection.
The UK does not currently operate a national prostate cancer screening programme, in contrast to breast and bowel cancer screening. This is because the evidence base for population-wide PSA screening producing a net survival benefit — when weighed against the harms of overdiagnosis and overtreatment of indolent cancers — has historically been mixed. However, the landscape is shifting. The TRANSFORM trial, launched in 2023, is the largest prostate cancer screening trial in history and aims to establish whether a national screening programme should be introduced.
In the meantime, men in the UK have the legal right to request a PSA test if they are aged 50 or over and have been fully counselled about what the test can and cannot tell them. This is called informed consent-based PSA testing, and it is available through your GP.
A single PSA result is rarely definitive. What matters more is the trend over time — whether PSA is rising and how quickly. Prostate cancer specialists often pay close attention to PSA velocity (the rate of change) as a signal of biological activity alongside absolute PSA levels.
Practical Takeaway
You do not need to wait for your GP to raise the subject of prostate health. You can request a PSA test if you are over 50 — or over 45 if you are in a higher-risk group. Ask for your result in absolute numbers and ask for it to be recorded so you have a baseline for future comparison. A single normal PSA is not a lifetime guarantee. Repeat testing at appropriate intervals is the standard of meaningful monitoring.
Prostate Health Risk Factors
| Non-Modifiable Risk Factors | Modifiable Risk Factors (Lifestyle) |
|---|---|
| Age: risk rises significantly after 50 | Body composition: excess body fat elevates oestrogen and promotes insulin resistance, both of which are associated with more aggressive prostate cancer |
| Family history: a father or brother with prostate cancer approximately doubles risk | Physical activity: regular exercise — particularly vigorous activity — is associated with reduced risk of advanced prostate cancer |
| Ethnicity: men of Black African or Caribbean heritage carry significantly higher lifetime risk | Diet: lycopene-rich foods, cruciferous vegetables, and soy isoflavones are associated with reduced prostate cancer risk in observational data |
| Genetic variants: BRCA2 and other gene mutations confer substantially elevated risk | Alcohol: heavy alcohol intake is associated with increased risk; moderate intake has less clear evidence |
| Height: taller men have modestly increased risk, possibly through IGF-1 signalling | Screening behaviour: early detection through PSA monitoring dramatically improves treatment options and outcomes |

Exercise and Prostate Health: What the Evidence Says
The relationship between physical activity and prostate cancer risk is one of the more robustly supported areas in the lifestyle oncology literature. A 2019 meta-analysis published in the British Journal of Sports Medicine examined over 140,000 men across 19 prospective cohort studies and found that high levels of physical activity were associated with a 10 percent reduction in overall prostate cancer risk and a significantly larger reduction — approximately 31 percent — in the risk of advanced or fatal prostate cancer.
The mechanisms are multiple. Regular exercise reduces circulating insulin and IGF-1, both of which can promote prostate cell proliferation. It reduces systemic inflammation, which contributes to tumour promotion. It improves metabolic health and reduces visceral adiposity, lowering the oestrogen excess associated with increased body fat. And there is emerging evidence that exercise may directly influence the tumour microenvironment, creating conditions less favourable to cancer progression.
For men with a prostate cancer diagnosis — particularly those on active surveillance or undergoing treatment — structured exercise is not merely beneficial but increasingly part of the clinical care model. Multiple randomised controlled trials have demonstrated that supervised exercise during and after prostate cancer treatment reduces fatigue, preserves lean mass (critical for men on androgen deprivation therapy, which dramatically accelerates muscle loss), improves quality of life, and reduces mortality from cardiovascular disease, which is a major competing cause of death in prostate cancer patients.
The evidence supports a combined approach of resistance training and aerobic exercise, with the former being particularly important for preserving muscle mass and bone density in men undergoing hormone-based treatments.
Practical Takeaway
If you have been diagnosed with prostate cancer and are undergoing or considering androgen deprivation therapy, a structured resistance training programme is not an optional extra — it is a clinical necessity. ADT-associated muscle loss and bone density reduction are serious side effects that exercise directly mitigates. If your oncologist has not raised this, raise it yourself and ask for a referral to an exercise physiologist or a fitness professional with oncology experience.
Nutrition and Prostate Health
The nutritional epidemiology of prostate cancer is complex and has, at times, produced conflicting results. However, several dietary factors have accumulated sufficient evidence to warrant practical attention.
Lycopene, the carotenoid responsible for the red colour of tomatoes, watermelon, and pink grapefruit, has been among the most extensively studied dietary compounds in relation to prostate health. A 2017 meta-analysis in the journal Medicine found an inverse association between lycopene intake and prostate cancer risk, with men in the highest lycopene intake tertile having approximately 12 percent lower risk. Notably, lycopene bioavailability is substantially higher from cooked or processed tomatoes than from raw — a finding that makes tinned tomatoes, tomato paste, and cooked tomato sauces more effective sources than fresh tomatoes consumed raw.
Soy isoflavones, particularly genistein and daidzein, have demonstrated anti-proliferative effects on prostate cancer cells in laboratory studies. Observational data from Asian populations — where prostate cancer rates are historically lower than in Western populations — have supported the hypothesis that habitual soy consumption is partially protective. The epidemiological signal has been replicated in several meta-analyses, though the effect size is modest and the evidence is not uniformly positive.
Cruciferous vegetables — broccoli, cauliflower, kale, Brussels sprouts, and cabbage — contain sulforaphane and indole-3-carbinol, compounds that have demonstrated anti-carcinogenic activity in prostate tissue. A prospective cohort study from EPIC found that men consuming cruciferous vegetables more than once per week had a reduced risk of localised prostate cancer compared to infrequent consumers.
Selenium and vitamin E have attracted considerable interest, though a large randomised controlled trial — the SELECT trial — found no benefit from supplementation with either in isolation. This is consistent with the broader nutritional principle that isolated nutrient supplementation frequently fails to replicate the effects observed with whole food consumption, where synergistic interactions between compounds are preserved.
High dairy consumption has been positively associated with prostate cancer risk in a number of large cohort studies, possibly through its effects on IGF-1, calcium metabolism, and the ratio of calcium to vitamin D. The evidence is not sufficient to recommend dairy elimination but warrants moderation in men at elevated risk.
Red and processed meat consumption has been associated with increased prostate cancer risk in multiple studies, with the strongest signal for processed meat. The mechanisms likely involve heterocyclic amines and polycyclic aromatic hydrocarbons produced during high-temperature cooking, as well as the high haem iron content of red meat.
Prostate-Supportive Nutrients
| Nutrient | Evidence Level | Best Plant-Based Sources | Best Omnivore Sources |
|---|---|---|---|
| Lycopene | Strong | Tinned tomatoes, tomato paste, tomato sauce, watermelon, pink grapefruit | Same sources. Universally applicable. |
| Soy isoflavones | Moderate to strong | Tofu, tempeh, edamame, soy milk, miso | Same sources. |
| Sulforaphane | Moderate | Broccoli, cauliflower, kale, Brussels sprouts, cabbage, rocket | Same. |
| Selenium | Moderate | Brazil nuts (1 to 2 per day), sunflower seeds, lentils, wholegrain bread | Fish, eggs, lean meat |
| Omega-3 fatty acids | Moderate | Algae oil, walnuts, flaxseed, chia seeds | Oily fish: salmon, mackerel, sardines |
| Vitamin E | Emerging | Sunflower seeds, almonds, hazelnuts, avocado, spinach | Same plant sources, also eggs |
Practical Takeaway
Adding cooked tomato products, cruciferous vegetables, and soy foods to your diet regularly is one of the most evidence-supported dietary actions a man can take for prostate health. You do not need exotic supplements. You need consistent inclusion of foods that are inexpensive, widely available, and supported by a substantial body of observational and mechanistic evidence. The nutritional pattern is broadly anti-inflammatory, plant-forward, and consistent with cardiovascular and metabolic health — the same dietary approach that benefits the rest of your health simultaneously.

How to Have the Conversation With Your GP
One of the most consistent barriers to prostate health action is discomfort initiating the conversation with a healthcare provider. Many men report feeling that they do not want to appear anxious, that they do not know what to ask, or that they are concerned about what might be found. These are understandable reactions. They are not useful ones.
Your GP will not judge you for raising prostate health. They will likely welcome it. A proactive, informed patient who asks specific questions is far easier to support than a patient who presents with advanced symptoms and no baseline history.
When you book an appointment specifically to discuss prostate health, tell the receptionist so that adequate time is allocated. When you are with your GP, be direct. Tell them your age, your risk factors (family history, ethnicity), and any symptoms you have noticed. Ask whether a PSA test is appropriate for you and, if so, what the result means in context. Ask what level would prompt further investigation and what follow-up intervals they recommend.
If your GP raises the topic of the limitations of PSA testing — which they are required to do as part of informed consent — listen to the full explanation, but do not allow it to become a reason not to test. Understanding the limitations of a test does not make the test worthless. A baseline PSA value, with repeat testing over time, provides information that no GP appointment without testing can provide.
Practical Takeaway
Write “ask about PSA test” on the notes on your phone right now. Not when you turn 50. Not when you notice a symptom. Now. If you are over 45 with a family history or you are of Black African or Caribbean heritage, make the appointment this week. The earlier the baseline, the more useful the trend data, and the earlier any significant change can be detected and investigated.
![Infographic titled 'What to Say · When to Say It · How to Make It Useful — The Prostate Conversation — six things to say at your GP appointment. In this order.' showing six numbered stacked rows with example phrasing: 01 Book the Right Appointment ('I'd like to book an appointment to discuss my prostate health — please allocate adequate time.'), 02 State Your Risk Profile ('I'm [age]. My father / brother had prostate cancer. I'm of Black African / Caribbean heritage.'), 03 Request the PSA Test ('I'd like to request a PSA test under informed consent.'), 04 Get Your Exact Number ('Please give me my PSA result in absolute numbers and record it on my file.'), 05 Ask for the Triggers ('At what PSA level would you recommend further investigation?'), 06 Schedule the Repeat ('What is the appropriate retesting interval for someone in my situation?'), closing 'A baseline today is the most useful number you can have. If you're over 45 with family history or Black African / Caribbean heritage — make the appointment this week. The earlier the baseline, the more useful the trend data.'](/_next/image?url=%2Fimages%2Fblog%2Fprostate-health%2Fimage-6.png&w=3840&q=75)
How I Work Alongside Men's Medical Care
My role is not to replace medical care or to provide medical advice. It is to optimise the lifestyle environment in which a man's medical care occurs. For men who are managing prostate conditions — whether active surveillance, BPH, post-treatment recovery, or simply proactive risk reduction — structured exercise and nutritional coaching provides a complementary layer of support that medicine alone cannot offer.
For men on active surveillance, I work to support the lifestyle factors that reduce progression risk: body composition, physical activity, nutrition, sleep, and stress. For men undergoing or recovering from treatment, I work to preserve or rebuild lean mass, maintain cardiovascular fitness, and address the hormonal consequences of therapy. For men who simply want to reduce their long-term risk and have never thought much about prostate health until now, I provide the framework to do so systematically.
This is not a niche area of coaching. It is central to what evidence-based health coaching for men over 40 should include. If prostate health is something you want to address as part of a broader coaching engagement, get in touch.
Work with Me
Get a personalised coaching plan built around your goals, your schedule, and your life.
Enquire NowReferences
- (1) Cancer Research UK. Prostate cancer statistics. Available at: cancerresearchuk.org [Accessed April 2025].
- (2) Prostate Cancer UK. Prostate cancer risk factors. Available at: prostatecanceruk.org [Accessed April 2025].
- (3) Leitão C, et al. Lycopene and prostate cancer: a systematic review of the literature. Nutrients. 2021.
- (4) Parsons JK, et al. Obesity, insulin resistance and prostate cancer: clinical and research implications. BJU International. 2008.
- (5) Wolin KY, et al. Physical activity and colon cancer prevention: a meta-analysis. British Journal of Cancer. 2009.
- (6) Giovannucci E, et al. A prospective study of physical activity and incident and fatal prostate cancer. Archives of Internal Medicine. 2005.
- (7) Newton RU, et al. Exercise medicine in the management of prostate cancer. Prostate Cancer and Prostatic Diseases. 2022.
- (8) Kang DW, et al. Effects of exercise on cancer-related fatigue and quality of life in men with prostate cancer. European Urology. 2021.
- (9) Key TJ, et al. Diet, nutrition and the prevention of cancer. Public Health Nutrition. 2004.
- (10) Richman EL, et al. Intakes of meat, fish, poultry, and eggs and risk of prostate cancer progression. American Journal of Clinical Nutrition. 2010.
- (11) Rowles JL, Erdman JW. Carotenoids and their role in cancer prevention. Biochimica et Biophysica Acta. 2020.
- (12) NHS England. Prostate cancer screening — PSA testing. Available at: nhs.uk [Accessed April 2025].
- (13) Lissowska J, et al. BRCA1 and BRCA2 mutations and prostate cancer: a systematic review and meta-analysis. European Journal of Cancer. 2015.
