
The Condition That Affects Millions of Women and Is Still Misunderstood
PCOS lifestyle management is a subject I come back to repeatedly in my coaching practice because polycystic ovary syndrome is one of the most common hormonal conditions in women of reproductive age, affecting between 5 and 10% of women globally, and it remains one of the most consistently mismanaged (1). The women who come to me having already been diagnosed with PCOS have, almost without exception, been told some version of the same inadequate advice: lose weight, exercise more, and consider the contraceptive pill. That is not a management strategy. It is a deflection.
What they have not been told is how insulin resistance drives the majority of PCOS presentations and why addressing that mechanism directly through resistance training, nutrition, and lifestyle is the most powerful intervention available. What they have not been told is why the standard advice to eat less and do more cardio is the worst possible approach for a woman whose metabolic environment makes weight management harder than it is for women without PCOS. What they have not been told is that meaningful improvement in symptoms, hormonal markers, and quality of life is achievable without necessarily reaching an idealised body weight.
This article gives you the explanation and the framework you should have been given at diagnosis.
What PCOS Actually Is and What the Cysts Are Not
Polycystic ovary syndrome is a hormonal and metabolic condition characterised by a combination of features including irregular or absent menstrual cycles, elevated androgens, and the presence of multiple small follicles on the ovaries. The name is a source of considerable confusion. The cysts are not cysts in the conventional sense. They are immature follicles, each containing an egg that has not reached full maturity and been released. They do not require surgical removal. They are a consequence of the underlying hormonal disruption, not a cause of it.
The diagnosis of PCOS is made using the Rotterdam criteria, which requires the presence of at least two of three features: irregular or absent ovulation, clinical or biochemical signs of elevated androgens such as excess facial or body hair, acne, or elevated testosterone on a blood test, and polycystic ovarian morphology on ultrasound. A woman can have PCOS without visible cysts on the ovaries, and a woman can have cysts without having PCOS. The name is genuinely misleading and has caused significant unnecessary anxiety (2).
Understanding what PCOS is at a mechanistic level matters because it determines why the lifestyle interventions I am about to describe work in the way they do. PCOS is not primarily a reproductive condition that happens to have metabolic consequences. For the majority of women with PCOS, it is a metabolic condition that manifests through reproductive disruption.
Top Tip
If you have been told you have polycystic ovaries on an ultrasound scan, this does not automatically mean you have PCOS. A formal diagnosis requires the presence of at least two of the three Rotterdam criteria. If you have concerns, ask your GP for a full hormonal blood panel including LH, FSH, testosterone, SHBG, fasting insulin, and fasting glucose alongside the ultrasound finding. A single scan result is not a diagnosis.
The Four PCOS Subtypes: Why One Approach Does Not Fit All
PCOS is not a single uniform condition. Research has identified four broad subtypes based on the features present, and the distinction matters for the lifestyle approach. Not all women with PCOS have insulin resistance, and not all have elevated androgens in clinically significant amounts. Treating every PCOS presentation identically misses this important nuance.
| Subtype | Key Features | Estimated Prevalence | Primary Lifestyle Priority |
|---|---|---|---|
| Type 1: Classic | Irregular cycles, elevated androgens, polycystic ovaries on scan. Most common and most severe presentation. | Most common: approximately 40 to 50% of diagnoses | Insulin resistance management is the primary target. Resistance training, low glycaemic load nutrition, adequate sleep and stress management. Inositol supplementation evidence relevant here. |
| Type 2: Androgen Excess Without Irregular Cycles | Regular cycles but elevated androgens: acne, excess hair, elevated testosterone. Often overlooked at diagnosis. | Approximately 20 to 30% of diagnoses | Anti-inflammatory nutrition, zinc, and saw palmetto (evidence limited but frequently used). Liver support through nutrition. Stress and cortisol management are particularly relevant here. |
| Type 3: Lean PCOS | All PCOS features but no insulin resistance or excess body weight. Often missed in initial assessment. | Approximately 15 to 20% of diagnoses | Stress and cortisol management most critical. Adequate nutrition, particularly avoiding undereating. Inflammatory drivers to investigate. Thyroid function check warranted. |
| Type 4: Post-Pill PCOS | Irregular cycles and sometimes androgen symptoms emerging after stopping hormonal contraception. Often temporary as the body re-establishes its own hormonal rhythm. | Approximately 10 to 15% of diagnoses | Patience and nutritional support for hormonal recovery. Seed cycling is popular though evidence is anecdotal. Nutrition adequacy and stress management. Often resolves within 3 to 6 months without further intervention. |
The subtype distinction is not always clear-cut and many women present with overlapping features. The lifestyle interventions in this article are broadly beneficial across all four types, with insulin resistance management being the most universally impactful target.
Insulin Resistance: The Central Mechanism Most Women Are Never Told About
For the majority of women with PCOS, insulin resistance is the metabolic engine driving the condition. Understanding this mechanism transforms the conversation from managing symptoms to addressing the underlying cause. And it explains precisely why the lifestyle interventions that improve insulin sensitivity, resistance training above all others, are so effective for PCOS.
When cells become resistant to insulin, the pancreas compensates by producing more. Chronically elevated insulin has a specific effect on the ovaries: it stimulates the ovarian theca cells to produce more androgens, particularly testosterone. Elevated androgens then disrupt the normal follicular development process, preventing eggs from maturing and being released, which produces the irregular or absent ovulation that characterises PCOS. The elevated androgens also produce the visible symptoms of acne, excess facial and body hair, and scalp hair thinning that cause significant distress for many women with PCOS (3).
The loop is self-reinforcing. Insulin resistance drives androgen excess. Androgen excess impairs follicular development and disrupts ovulation. Disrupted ovulation means inadequate progesterone production in the second half of the cycle, which worsens oestrogen dominance, which further impairs insulin sensitivity. Each element feeds the next.
This is why approaches that improve insulin sensitivity directly break the cycle at its root. Resistance training activates GLUT4 glucose transporters in muscle cells, improving the cell's ability to absorb glucose without requiring elevated insulin. Fat loss from the visceral depot reduces the inflammatory signals that drive insulin resistance. Low glycaemic load nutrition stabilises blood glucose and reduces the chronic insulin demand that keeps the cycle turning.
The PCOS Hormonal Loop: How Insulin Resistance Drives the Cycle
THE PCOS INSULIN-ANDROGEN LOOP
01
Insulin Resistance
Cells respond poorly to insulin.
02
Pancreas Compensates
Higher insulin output. Fasting insulin rises.
03
Ovarian Overproduction
Elevated insulin stimulates the ovarian theca cells to overproduce androgens, particularly testosterone.
04
Ovulation Disrupted
Elevated androgens prevent follicles from maturing normally. Ovulation is disrupted or absent.
05
Progesterone Falls
Progesterone production falls. Oestrogen dominance worsens. Symptoms emerge: irregular cycles, acne, excess hair, hair loss.
06
The Loop Tightens
Androgen excess and oestrogen dominance further impair insulin sensitivity. The cycle compounds.
Without intervention, the cycle compounds. With the right lifestyle intervention, it can be interrupted at multiple points.
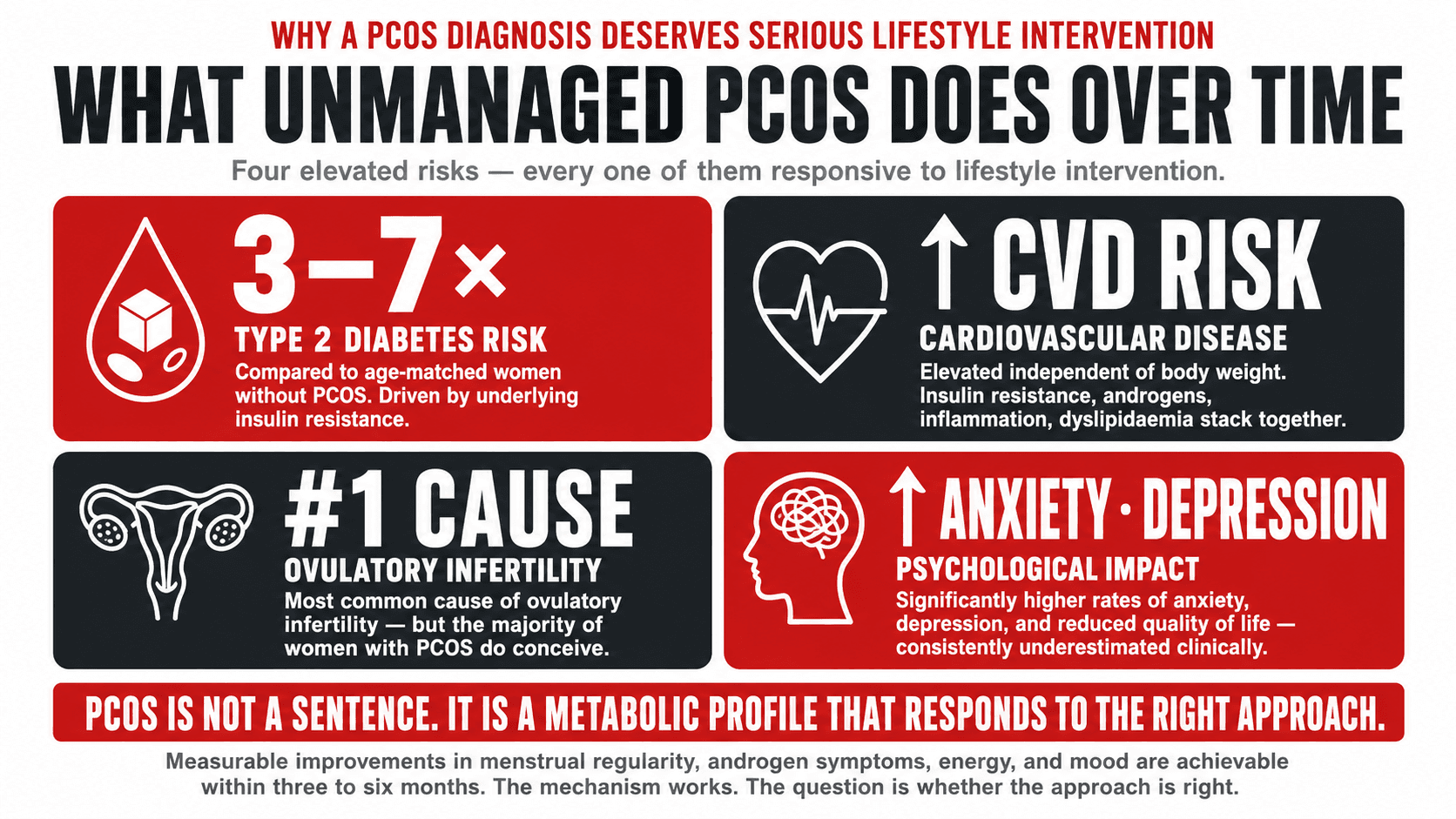
What Happens When PCOS Is Left Unmanaged
I am not going to describe the consequences of unmanaged PCOS to frighten you. I am going to describe them because every woman with this diagnosis deserves to understand the full picture so she can make genuinely informed decisions about how seriously to take it.
Type 2 diabetes risk is substantially elevated in women with PCOS. Research has found that women with PCOS have a significantly higher prevalence of impaired glucose tolerance and Type 2 diabetes compared to age-matched women without the condition, with some studies estimating a three to seven times higher risk (4). This is a direct consequence of the insulin resistance that characterises the majority of PCOS presentations. It is preventable through the same lifestyle interventions that manage PCOS symptoms.
Cardiovascular risk is also elevated in women with PCOS, independent of body weight. The combination of insulin resistance, elevated androgens, chronic low-grade inflammation, and the dyslipidaemia that frequently accompanies PCOS creates a cardiovascular risk profile that requires active management rather than passive monitoring.
The psychological impact of PCOS is consistently underestimated in clinical settings. Research published in the journal Human Reproduction found that women with PCOS have significantly higher rates of anxiety, depression, and reduced quality of life compared to women without the condition, driven by a combination of visible symptoms, infertility concerns, and the chronic nature of the condition (5). The physical and psychological dimensions of PCOS are inseparable, and any management strategy that addresses one without the other is incomplete.
Fertility, while not a concern for every woman with PCOS, is frequently affected. PCOS is the most common cause of ovulatory infertility. However, it is important to note that the majority of women with PCOS do conceive, often with relatively modest lifestyle intervention, and infertility is not an inevitable outcome of the diagnosis.
Top Tip
A PCOS diagnosis is not a sentence. It is a metabolic profile that responds meaningfully to the right lifestyle intervention. The women I have coached with PCOS who committed to a structured resistance training programme and a protein-rich, low glycaemic load nutrition strategy experienced measurable improvements in menstrual regularity, androgen symptoms, energy, and mood within three to six months. The mechanism works. The question is whether the approach is right.
Resistance Training: The Most Important Lifestyle Intervention for PCOS
Of all the lifestyle interventions available for PCOS, resistance training is the one with the strongest and most consistent evidence base, and the one most commonly absent from the advice women with PCOS receive. Walking is recommended. Yoga is suggested. Resistance training, which directly addresses the insulin resistance that drives the majority of PCOS presentations, is rarely the centrepiece of the conversation.
The mechanism is specific. Skeletal muscle is the largest insulin-sensitive tissue in the body. When muscle cells contract during resistance exercise, they activate GLUT4 glucose transporters that allow glucose to enter the cell independently of insulin. Over time, consistent resistance training increases the number and sensitivity of these transporters, improving insulin sensitivity in the most direct way available without medication. Research published in Fertility and Sterility demonstrated that resistance training significantly reduced fasting insulin, testosterone, and waist circumference in women with PCOS, independent of weight loss (6).
Building more muscle mass through progressive resistance training amplifies this benefit further. Greater muscle mass represents a larger glucose-absorbing tissue pool, meaning that the same carbohydrate load produces a smaller blood glucose and insulin response in a more muscular woman than in a less muscular one. This is a structural metabolic improvement that accumulates over months and years of consistent training.
Three to four resistance training sessions per week, structured around compound movements that recruit the largest muscle groups, including squats, deadlifts, hip hinges, rows, and presses, is the framework I build for women with PCOS. Intensity should be meaningful: the last two to three repetitions of each set should require genuine effort. This is not gentle movement. It is metabolic medicine.
Top Tip
If you have PCOS and you are currently doing primarily cardio-based exercise, I am not suggesting you stop. I am suggesting that you make resistance training the foundation of your programme and treat cardio as a complement to it. The metabolic benefit of building and maintaining muscle tissue is the most powerful lifestyle lever available for insulin resistance. Post-meal walking for twenty minutes is also highly effective for blunting blood glucose and insulin responses after eating and requires no gym access.

Nutrition for PCOS: What the Evidence Supports
The nutritional strategy for PCOS is built on three non-negotiable foundations: blood glucose stability, adequate protein, and anti-inflammatory food quality. These are not competing priorities. They reinforce one another when the approach is designed correctly.
Low glycaemic load eating is the most consistently supported nutritional approach in the PCOS literature. A low glycaemic load diet reduces the blood glucose peaks that drive insulin spikes, which directly reduces the ovarian stimulation that drives androgen production. This does not mean eliminating carbohydrates. It means replacing refined, rapidly absorbed carbohydrates with whole food alternatives that produce a slower, lower blood glucose response. Oats, lentils, chickpeas, sweet potato, brown rice, quinoa, and non-starchy vegetables are the foundations of a PCOS-friendly carbohydrate strategy. Ultra-processed foods, white bread, sugary drinks, and refined snack foods are the primary targets for reduction (7).
Protein at every meal is essential for blood glucose stability, satiety, and muscle protein synthesis. Targeting 1.6 to 2 grams of protein per kilogram of bodyweight per day is appropriate for most women with PCOS engaged in resistance training. For plant-based women, tofu, tempeh, seitan, edamame, soy protein, pea protein, lentils, chickpeas, and black beans are the building blocks of a protein strategy that meets this target without requiring animal products. Distributing protein across three to four meals rather than concentrating it in one or two is more effective for blood glucose management.
Dietary fat quality matters significantly in PCOS. Omega 3 fatty acids from oily fish, or algae oil for plant-based women, walnuts, flaxseed, and chia seeds have anti-inflammatory properties that are directly relevant to the chronic low-grade inflammation that characterises PCOS. Replacing saturated fat from highly processed sources with monounsaturated fats from olive oil, avocado, and nuts improves the inflammatory and lipid profile that PCOS tends to worsen.
A specific note on soy for women with PCOS: the concern that phytoestrogens in soy might worsen hormonal conditions in women is not supported by the evidence at normal dietary intake levels. Research has consistently found that moderate soy consumption does not disrupt the female hormonal environment and may have mild anti-androgenic properties that are potentially beneficial in PCOS (8). Tofu, tempeh, edamame, and soy protein are safe and nutritionally valuable choices for women with PCOS.
Top Tip
The most impactful single nutritional change for the majority of women with PCOS is building every meal around a substantial protein source and replacing refined carbohydrates with whole food alternatives. This does not require a special diet, a restricted eating window, or eliminating any food group. It requires structure: protein first, whole food carbohydrates, plenty of non-starchy vegetables, and quality fats. Applied consistently, this pattern reduces blood glucose volatility and insulin demand directly at the dietary level.

Inositol: What the Evidence Actually Says
Myo-inositol and D-chiro-inositol are two forms of a naturally occurring compound that plays a role in insulin signalling. They have attracted significant research interest in the context of PCOS because of their potential to improve insulin sensitivity, reduce androgen levels, support ovulation, and improve egg quality in women undergoing fertility treatment. The evidence is genuinely encouraging.
A meta-analysis published in the European Review for Medical and Pharmacological Sciences found that myo-inositol supplementation significantly improved insulin resistance, testosterone levels, and menstrual regularity in women with PCOS (9). The combination of myo-inositol and D-chiro-inositol in a 40:1 ratio, which approximates the physiological ratio found in most tissues, has shown the most consistent results across research. A typical dose used in trials is 2 grams of myo-inositol twice daily.
Dietary sources of inositol include wholegrains, particularly oats and brown rice, legumes, nuts, and citrus fruits. Supplemental inositol is widely available, generally well-tolerated, and relatively inexpensive. It is not a replacement for the lifestyle interventions described in this article. It is a useful addition that sits on top of a solid foundation.
I always recommend discussing supplementation with your GP or a registered dietitian before beginning, particularly if you are taking any medication or undergoing fertility treatment. Inositol has an excellent safety record but individual clinical circumstances vary.
Top Tip
If you are considering inositol supplementation, look for a product containing myo-inositol and D-chiro-inositol in a 40:1 ratio. Take it with food to reduce any gastrointestinal discomfort. Give it a minimum of three months before assessing its effect on cycle regularity and symptoms, as the hormonal picture takes time to shift. Inositol is widely available in the UK and does not require a prescription.
Sleep, Stress, and Cortisol in PCOS: The Variables That Training Cannot Compensate For
Chronic stress and poor sleep are two of the most significant and least discussed drivers of PCOS symptom severity, and they operate through the same cortisol-insulin axis that resistance training and nutrition seek to improve. If training and nutrition are well-managed but sleep is inadequate and stress is sustained and unaddressed, the hormonal environment of PCOS will remain compromised.
Cortisol directly stimulates androgen production in the adrenal glands through a pathway distinct from the ovarian mechanism described earlier. In women with PCOS who are under chronic stress, this adrenal androgen contribution adds to the ovarian androgen excess, worsening symptoms and further disrupting the menstrual cycle. Research has demonstrated that women with PCOS have higher baseline cortisol levels and a more pronounced cortisol response to stress than women without the condition (10).
Poor sleep worsens insulin resistance within days through mechanisms described in detail in the sleep article in this series. For women with PCOS, who are already insulin resistant, even modest sleep restriction compounds the metabolic picture significantly. Seven to eight hours of quality sleep per night is not a lifestyle preference for women with PCOS. It is a clinical priority.
The practical stress management tools that are most relevant here are the same ones that apply to any woman: consistent sleep and wake times, scheduled recovery from training, deliberate disengagement from work in the evening hours, post-meal walking, and where appropriate, structured relaxation practices such as diaphragmatic breathing. None of these are soft recommendations. They are physiological interventions with measurable hormonal consequences.
Top Tip
If your PCOS symptoms worsen significantly during periods of high stress, this is the HPA axis and adrenal androgen production telling you directly that the stress load is affecting your hormonal environment. Track your symptoms relative to your stress levels for one to two months. The pattern will almost certainly be clear. That awareness is the first step toward managing it with the seriousness it warrants.
Your PCOS Management Framework
Managing PCOS Through Lifestyle — The Three-Part Framework
Resistance Training
- • 3 to 4 sessions per week
- • Compound movements: squats, deadlifts, rows, presses
- • Progressive overload over time
- • Post-meal walking 20 minutes
- • GLUT4 activation: bypasses broken insulin pathway
- • Builds the muscle mass that improves metabolic rate
Nutrition
- • Protein 1.6 to 2g per kg per day
- • Low glycaemic load carbohydrates: oats, lentils, sweet potato, quinoa
- • Omega 3: oily fish or algae oil, walnuts, flaxseed
- • Anti-inflammatory diet quality
- • No need to eliminate food groups
- • Consider myo-inositol: 2g twice daily with food
Sleep and Stress
- • 7 to 8 hours per night, non-negotiable
- • Consistent wake time seven days per week
- • Identify and address the primary stress sources
- • Diaphragmatic breathing: 5 minutes daily
- • Scheduled training recovery and deload weeks
- • Track symptoms relative to stress: the pattern will be clear
These three pillars work together. Resistance training improves insulin sensitivity. Nutrition reduces the blood glucose demand that drives insulin excess. Sleep and stress management reduce the cortisol and adrenal androgen contributions that worsen the hormonal picture. All three simultaneously produce the most meaningful change.
When to Talk to Your GP: Medical Management of PCOS
Lifestyle intervention is the foundation of PCOS management and in many cases produces sufficient improvement to control symptoms and reduce long-term health risks without medication. However, there are clinical situations where medical intervention is appropriate and where lifestyle alone is insufficient.
Metformin, an insulin-sensitising medication primarily used in Type 2 diabetes management, is used in PCOS to improve insulin resistance, reduce androgen production, and support menstrual regularity. It is not a first-line treatment in the UK but is often appropriate for women with confirmed insulin resistance or prediabetes alongside PCOS. The combination of Metformin and lifestyle intervention produces better outcomes than either alone.
The combined oral contraceptive pill is frequently prescribed for PCOS to regulate cycles and manage androgen-driven symptoms including acne and excess hair growth. It is effective for symptom management but does not address the underlying metabolic condition. Women using the pill for PCOS management should understand that it suppresses the hormonal cycle rather than correcting it, and that symptoms typically return after stopping if the underlying insulin resistance has not been addressed.
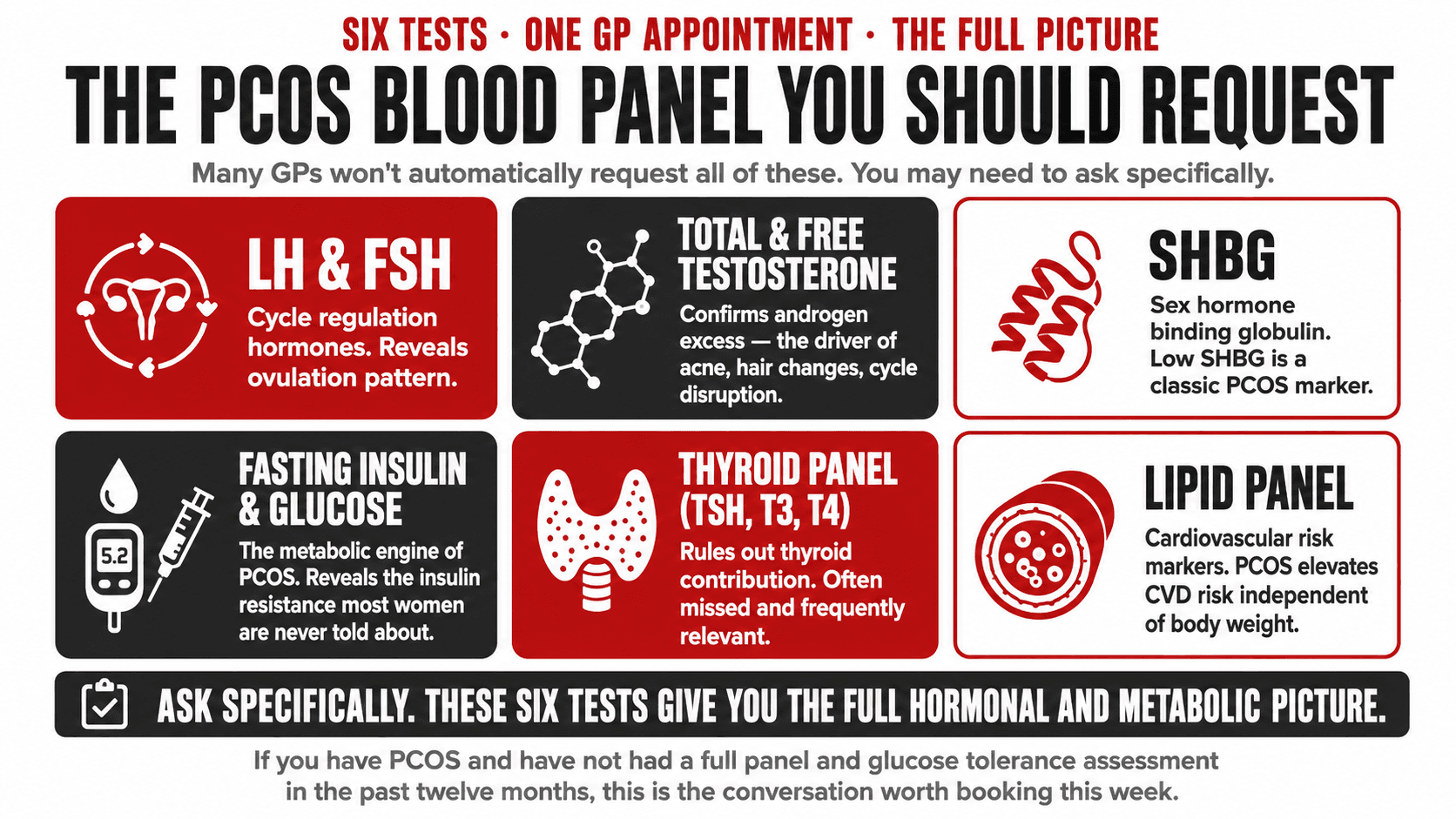
Anti-androgen medications, thyroid assessment where relevant, and fertility treatment in women trying to conceive are all areas requiring clinical input. If you have PCOS and have not had a full hormonal panel, fasting insulin, and glucose tolerance assessment in the past twelve months, requesting these from your GP is a reasonable and important first step.
Top Tip
Ask your GP specifically for: LH and FSH levels, total and free testosterone, SHBG (sex hormone binding globulin), fasting insulin, fasting glucose or HbA1c, thyroid function tests, and a lipid panel. These six test categories give a comprehensive baseline picture of your PCOS hormonal and metabolic profile. Many GPs will not automatically request all of these. You may need to ask specifically.
How I Work With Women With PCOS
PCOS is one of my core specialisms and one I approach with particular care because the condition sits at the intersection of metabolic health, hormonal health, and psychological wellbeing in a way that requires a genuinely integrated response. I do not treat PCOS. I work with the lifestyle variables that the evidence supports as the most powerful determinants of PCOS symptom severity and metabolic risk.
The women I have coached with PCOS who committed to a structured resistance training programme, a protein-rich low glycaemic load nutrition strategy, and the sleep and stress foundations described in this article have experienced measurable improvements in menstrual regularity, androgen symptoms, energy, body composition, and mood within three to six months. The biology works when the approach is correct.
If you have PCOS and are ready to address it with the seriousness and precision it warrants, I work one-to-one with women online globally. The programme I build will be designed around your specific subtype, your health history, your dietary background, and your life. Every element of it will be evidence-based and calibrated to the actual mechanisms of your condition.
