Men's heart health is the single most important topic in men's health, and it is also the one most men do the least about until they have no choice. Cardiovascular disease is the leading cause of death in men across the UK, Europe, and North America. It kills more men than all cancers combined. And yet the majority of men I speak to have never had their blood pressure measured outside of a GP visit for something unrelated, have no idea what their cholesterol numbers are, and could not tell you what their resting heart rate is.
This is not a problem of intelligence or willpower. It is a problem of awareness. Men are not taught to think about their cardiovascular health until the consequences of ignoring it become impossible to avoid. A heart attack. A stroke. A diagnosis that arrives with a list of medications and a set of restrictions that significantly alter the life they had planned. This article exists to give you the knowledge you need before you reach that point.
I am going to walk you through the numbers that matter, explain what they mean in plain English, and show you exactly how your training, nutrition, and lifestyle choices are either protecting your cardiovascular system or eroding it. Cardiovascular health is the foundation on which everything else is built. Get this right, and everything else becomes more achievable.
The Men's Heart Health Crisis Nobody Talks About
In the United Kingdom, cardiovascular disease causes around 160,000 deaths every year. Men account for a disproportionate share of those deaths, particularly in middle age. According to the British Heart Foundation, men under 75 are significantly more likely to die from coronary heart disease than women of the same age. In the United States, the Centers for Disease Control and Prevention reports that one in four male deaths is caused by heart disease.
What makes this crisis so insidious is that the underlying pathology develops silently over decades. Atherosclerosis, the gradual narrowing and hardening of the arteries caused by the build-up of fatty plaques, begins in many cases during a man's 20s. It progresses through his 30s and 40s without producing any noticeable symptoms. By the time a man reaches his 50s, the damage can be substantial, and the first symptom he experiences is sometimes a heart attack.
The tragedy is that this is largely preventable. The major risk factors for cardiovascular disease, including high blood pressure, elevated LDL cholesterol, elevated triglycerides, excess visceral fat, insulin resistance, and physical inactivity, are all modifiable. They respond to lifestyle intervention. But intervention requires awareness, and awareness requires the right information delivered at the right time. That is what this article is designed to provide.
Why Men Are at Greater Risk
Women have a degree of cardiovascular protection from oestrogen during their reproductive years. Oestrogen supports healthy lipid profiles by raising HDL cholesterol, maintaining arterial flexibility, and exerting anti-inflammatory effects on blood vessel walls. Men do not have this protection to the same degree. The result is that men develop cardiovascular disease approximately 10 years earlier than women, and the risk escalates more steeply from the age of 45 onwards.
Men also tend to accumulate visceral fat, the metabolically active fat stored around the internal organs, more readily than pre-menopausal women. Visceral fat is not passive tissue. It produces inflammatory cytokines, disrupts insulin signalling, raises triglycerides, and directly contributes to arterial inflammation. It is both a marker and a driver of cardiovascular risk.
There is also a behavioural dimension. Men are less likely to attend routine health checks, less likely to act on warning signs, and less likely to seek medical help proactively. In a 2019 survey by the British Medical Journal, men were found to be 24 percent less likely than women to have seen a GP in the previous year. This means that conditions that could be caught and managed early are instead allowed to progress unchecked.
Blood Pressure: The Silent Killer Explained Simply
Hypertension, or high blood pressure, is the single most significant modifiable risk factor for cardiovascular disease, stroke, and kidney disease. It is called the silent killer because it produces no symptoms in the vast majority of cases. You can have dangerously elevated blood pressure for years without feeling any different. The first sign is often a catastrophic cardiovascular event.
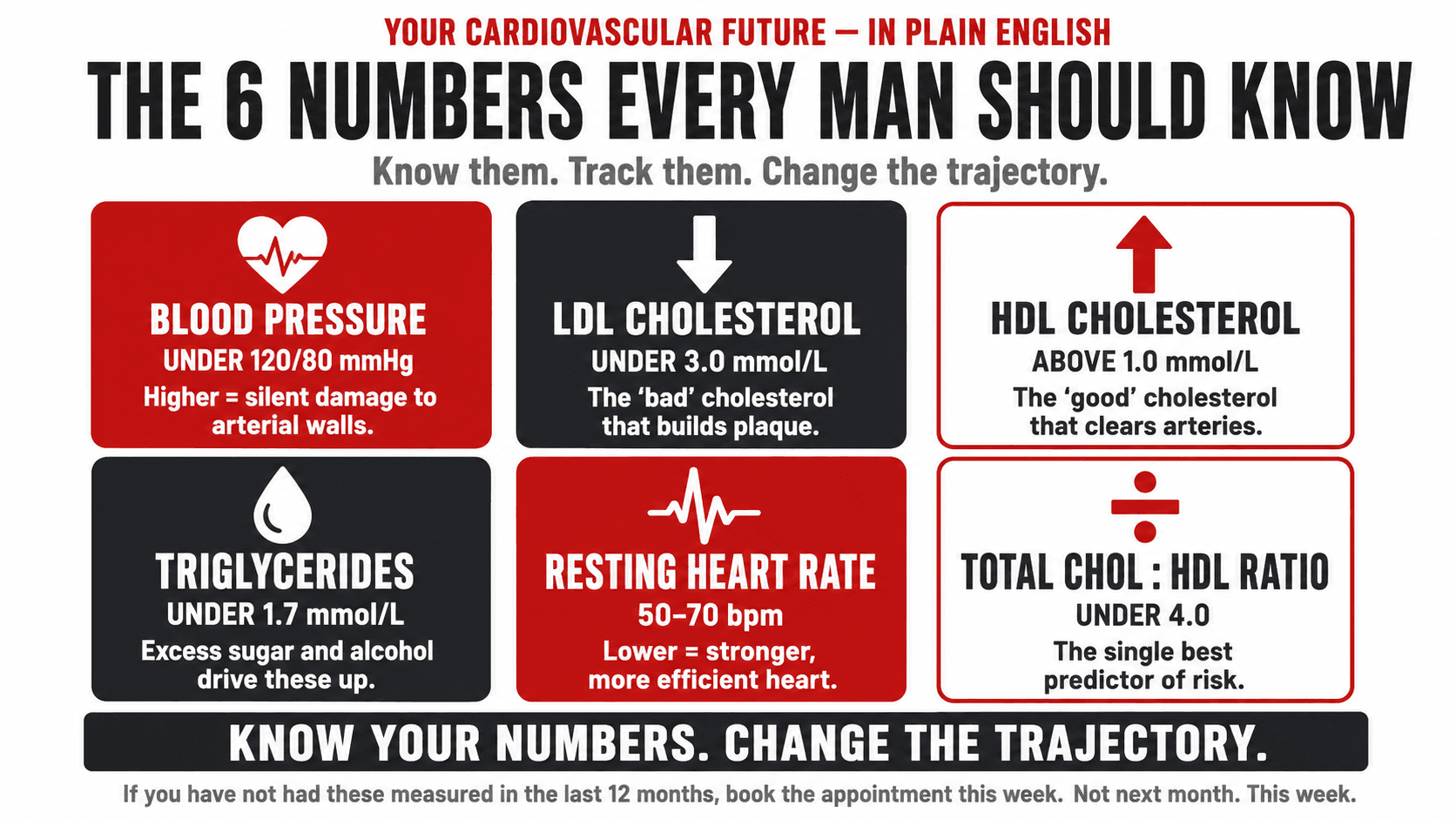
Blood pressure is measured as two numbers. The first, systolic pressure, represents the pressure in your arteries when your heart beats. The second, diastolic pressure, represents the pressure when your heart rests between beats. A reading of 120 over 80 millimetres of mercury is considered optimal. Readings above 140 over 90 are classified as hypertension and require medical attention.
Chronically elevated blood pressure damages the walls of the arteries over time. This damage accelerates atherosclerosis, increases the likelihood of arterial plaques rupturing, and significantly raises the risk of both heart attack and stroke. The good news is that blood pressure responds remarkably well to lifestyle intervention. Regular cardiovascular exercise, resistance training, reduced sodium intake, increased dietary potassium, reduced alcohol consumption, and weight loss in those who carry excess weight can all produce clinically meaningful reductions in blood pressure without medication, particularly in the early to moderate stages of hypertension.
Top Tip
Book a health check with your GP and specifically ask for blood pressure measurement, fasting blood glucose, a full lipid panel including LDL, HDL, and triglycerides, and a resting heart rate. If you are over 40 and have not had these measurements taken in the last 12 months, book the appointment this week. Not next month. This week.
Cholesterol: What Your GP Is Actually Measuring
Cholesterol is not a poison. It is a lipid molecule that your body produces and needs for building cell membranes, producing hormones, and synthesising vitamin D. The problem arises when certain forms of cholesterol are present in excess and in an environment of arterial inflammation.
When your GP measures your cholesterol, they are typically looking at several distinct markers. Total cholesterol gives a broad overview but is a poor predictor of cardiovascular risk when considered in isolation. LDL cholesterol, often referred to as the bad cholesterol, is the primary lipoprotein responsible for depositing cholesterol into arterial walls and initiating plaque formation. HDL cholesterol, often called the good cholesterol, performs the reverse function: it transports cholesterol away from the arteries and back to the liver for processing. Triglycerides are a form of fat found in the blood, elevated levels of which independently predict cardiovascular risk, particularly in men with metabolic syndrome or insulin resistance.
The ratio of total cholesterol to HDL is increasingly recognised as one of the most clinically useful single markers. A ratio below 4.0 is associated with low cardiovascular risk. A ratio above 5.0 indicates elevated risk and warrants investigation and intervention.
Top Tip
If you own a home blood pressure monitor, take three readings in the morning before eating, drinking, or taking any medication. Sit quietly for five minutes first. Record all three and take the average. This gives you a more accurate picture than a single GP reading taken in a clinical setting where anxiety can temporarily elevate the result.
Resting Heart Rate: The Number Most Men Never Check
Your resting heart rate is the number of times your heart beats per minute when you are completely at rest. It is one of the simplest and most accessible markers of cardiovascular fitness and autonomic nervous system health. A lower resting heart rate generally indicates a more efficient heart that pumps more blood per beat and does not need to work as hard to maintain circulation at rest.
Elite endurance athletes commonly have resting heart rates in the low 40s or even high 30s. For the general population, a resting heart rate between 50 and 70 beats per minute is considered healthy. A resting heart rate consistently above 80 beats per minute, and particularly above 100 beats per minute, which is defined as tachycardia, is associated with increased cardiovascular risk, and may indicate deconditioning, high stress levels, thyroid dysfunction, anaemia, or other underlying issues that warrant investigation.
The encouraging reality is that resting heart rate is highly responsive to aerobic conditioning. Consistent cardiovascular exercise, whether walking, cycling, swimming, or rowing, will lower your resting heart rate over weeks and months as your heart becomes more efficient. This is one of the clearest and most directly measurable signs that your cardiovascular system is improving.
Top Tip
Ask your GP for your full lipid panel, not just your total cholesterol. Specifically request your LDL, HDL, triglycerides, and total cholesterol to HDL ratio. Understanding these individual numbers gives you a far more accurate picture of your cardiovascular risk than total cholesterol alone, which can be misleadingly reassuring in some cases and misleadingly alarming in others.
Your Heart Health Numbers at a Glance
| Marker | Healthy Range | At-Risk Range | Danger Range | What to Do |
|---|---|---|---|---|
| Blood Pressure | Under 120/80 mmHg | 120–139 / 80–89 mmHg | 140/90 mmHg or above | See GP, review training and nutrition, reduce sodium, increase potassium |
| LDL Cholesterol | Under 3.0 mmol/L | 3.0 to 4.0 mmol/L | Above 4.0 mmol/L | Review saturated fat intake, increase fibre, discuss medication options with GP |
| HDL Cholesterol | Above 1.0 mmol/L (men) | 0.9 to 1.0 mmol/L | Below 0.9 mmol/L | Increase cardio, add omega 3, reduce refined carbohydrates, quit smoking |
| Triglycerides | Under 1.7 mmol/L | 1.7 to 5.6 mmol/L | Above 5.6 mmol/L | Reduce sugar and alcohol, increase omega 3 and fibre, exercise consistently |
| Resting Heart Rate | 50 to 70 bpm | 70 to 85 bpm | Above 100 bpm at rest | Begin consistent cardiovascular training, check for underlying thyroid issues with GP |
| Total Cholesterol to HDL Ratio | Under 4.0 | 4.0 to 5.0 | Above 5.0 | Improve overall lipid profile through training, nutrition, and GP review |

How Resistance Training Protects the Cardiovascular System
There is a persistent misconception that cardiovascular health is exclusively the domain of cardiovascular exercise. The image of the heart-healthy person is someone running, cycling, or swimming, not someone doing squats or pressing a barbell overhead. The science tells a more nuanced and considerably more interesting story.
Resistance training produces a distinct and complementary set of cardiovascular adaptations that aerobic exercise alone does not fully replicate. A meta-analysis published in the British Journal of Sports Medicine in 2019, which analysed data from over 1.2 million participants, found that muscle-strengthening activities were independently associated with a 17 percent reduction in cardiovascular disease risk, a 12 percent reduction in all-cause mortality, and a 10 percent reduction in cancer mortality, even after controlling for aerobic exercise.
The mechanisms behind this are multiple. Resistance training improves insulin sensitivity, which reduces the glucose-driven damage to arterial walls that underlies much of cardiovascular disease progression. It reduces visceral fat more effectively than aerobic exercise in some populations. It improves arterial stiffness over time. It reduces resting blood pressure in hypertensive individuals. And it builds the skeletal muscle mass that acts as a glucose reservoir, reducing the metabolic conditions that drive cardiovascular risk.
Top Tip
You do not need to choose between weights and cardio. For cardiovascular protection, you need both. The research is consistent: the combination of resistance training and aerobic exercise produces superior outcomes for blood pressure, lipid profiles, blood glucose, and cardiovascular risk reduction compared to either modality alone. Aim for at least two resistance training sessions and two moderate-intensity cardiovascular sessions per week as a minimum foundation.
How Exercise Protects Your Heart
| Resistance Training | Cardiovascular Exercise |
|---|---|
| Improves insulin sensitivity and reduces blood glucose | Lowers resting heart rate over time |
| Reduces visceral fat accumulation | Improves VO2 max and cardiac output |
| Reduces resting blood pressure in hypertensive individuals | Reduces blood pressure through arterial compliance |
| Builds glucose-storing skeletal muscle mass | Lowers triglycerides directly |
| Modestly raises HDL cholesterol | Raises HDL cholesterol more substantially |
| Reduces arterial stiffness over long-term training | Strengthens the heart muscle directly |
| Reduces systemic inflammation markers | Improves endothelial (arterial wall) function |

The Silent Progression Timeline
| Age | What Is Typically Happening |
|---|---|
| 20s | Early fatty streak formation in arterial walls is already detectable at autopsy in many young men, particularly those with poor diet, high stress, or smoking history. No symptoms. No awareness. The process begins silently. |
| 30s | Visceral fat begins to accumulate if lifestyle is sedentary. LDL deposits build on existing arterial lesions. Blood pressure may begin a slow upward trend. Insulin sensitivity starts declining without resistance training. Still no symptoms in most men. |
| 40s | Blood pressure often becomes measurably elevated for the first time. Arterial plaques are now established. Testosterone begins declining, which further accelerates visceral fat gain and reduces the natural anti-inflammatory protection testosterone provides to arterial walls. Risk escalates significantly. |
| 50s | Arterial stiffness is now measurable. Blood pressure is often established as hypertension requiring medication. Plaque burden is significant. The first cardiovascular events often occur in this decade in men who have not intervened. The window for effortless lifestyle-only correction is narrowing. |
Nutrition and Heart Health
The relationship between diet and cardiovascular health is one of the most studied areas in all of nutritional science, and the key findings are considerably more nuanced than the oversimplified messaging most men have absorbed over the years. The old narrative that dietary fat causes heart disease has been substantially revised. The current evidence points to a more complex picture involving the quality of fats consumed, the overall dietary pattern, and the metabolic context in which nutrients are eaten.
What the evidence consistently supports is this: a dietary pattern high in minimally processed whole foods, rich in fibre, omega-3 fatty acids, potassium, polyphenols, and adequate protein, while low in ultra-processed foods, refined sugars, excess sodium, and trans fats, is strongly associated with reduced cardiovascular risk. This is not a single diet. It describes the Mediterranean pattern, elements of the DASH diet, and any well-constructed whole-food approach regardless of macronutrient distribution.
For men specifically, the nutrients most reliably associated with cardiovascular protection are soluble fibre for LDL reduction, omega-3 fatty acids for triglyceride and inflammation management, potassium for blood pressure regulation, and polyphenols from plant foods for endothelial protection.
Top Tip
Add a portion of oats to your breakfast and a serving of legumes to at least one meal per day. These two changes alone, if sustained, can produce a clinically meaningful reduction in LDL cholesterol over eight to twelve weeks. Oats contain beta-glucan, a soluble fibre that binds to cholesterol in the digestive tract and removes it from circulation. Legumes provide a combination of soluble fibre and potassium that supports both cholesterol and blood pressure management simultaneously.
Heart-Protective Foods
| Food | Key Nutrient | Cardiovascular Benefit | Omnivore Source | Plant-Based Source |
|---|---|---|---|---|
| Oats | Beta-glucan | Reduces LDL cholesterol | Porridge | Same |
| Lentils and legumes | Soluble fibre, potassium | Lowers LDL and blood pressure | Add to soups | Cornerstone of plant-based diet |
| Oily fish | EPA and DHA omega 3 | Reduces triglycerides | Salmon, mackerel, sardines | Algae oil supplement |
| Walnuts and flaxseed | ALA omega 3, fibre | Anti-inflammatory | Snacking | Same |
| Sweet potato and spinach | Potassium, folate | Blood pressure regulation | As a side dish | Same |
| Olive oil | Monounsaturated fat, polyphenols | Reduces LDL oxidation | Cooking oil | Same |
| Tofu and tempeh | Soy protein, isoflavones | Modest LDL reduction | Protein substitute | Primary protein source |
Alcohol and the Heart
Alcohol and cardiovascular health is one of the most frequently misrepresented topics in popular health media. For decades, observational research appeared to suggest that moderate alcohol consumption, particularly red wine, was associated with reduced cardiovascular risk. This created a widely held belief that drinking in moderation was either neutral or mildly protective for the heart.
The more recent and methodologically rigorous evidence has substantially revised this position. Mendelian randomisation studies, which use genetic variants to eliminate confounding factors that distort observational data, have consistently found that alcohol consumption has no cardioprotective effect and that the apparent benefits seen in earlier studies were artefacts of confounding. People who drink moderately tend to have other lifestyle characteristics associated with better health. When those confounders are controlled for, the protective effect of alcohol disappears.
What is clear from the evidence is this: alcohol raises blood pressure in a dose-dependent manner, raises triglycerides, contributes to visceral fat accumulation, disrupts sleep architecture in ways that increase cardiovascular risk, and raises the risk of atrial fibrillation, which is a significant independent cardiovascular risk factor. For men who drink regularly, even at levels that society considers moderate, reducing intake is one of the most high-impact single changes they can make for their cardiovascular health.
Top Tip
If you drink regularly, even at what you consider moderate levels, reducing your intake is one of the most impactful single changes you can make for your cardiovascular health. You do not need to become teetotal to see benefit. Moving from daily drinking to three or four occasions per week, and reducing volume per occasion, will produce measurable improvements in blood pressure and triglycerides within four to eight weeks.
When to Get a Health Check
If you are a man over the age of 35 and you have not had your blood pressure, fasting blood glucose, and full lipid panel measured in the last 12 months, you should arrange a health check as a matter of priority. This is not alarmist. It is simply the responsible application of available medical tools to catch developing problems before they become established ones.
In the UK, the NHS Health Check programme offers free cardiovascular risk assessments to adults between the ages of 40 and 74. It includes blood pressure measurement, cholesterol testing, blood glucose assessment, and a BMI calculation. If you have not used this service, contact your GP surgery to arrange it. If you are under 40 but have a family history of cardiovascular disease, hypertension, or type 2 diabetes, arrange a conversation with your GP about earlier screening.
Beyond formal health checks, certain symptoms warrant immediate medical attention. Chest pain or tightness, shortness of breath on exertion that is new or worsening, persistent unexplained fatigue, palpitations, or episodes of dizziness or near-fainting should all be evaluated promptly. These may or may not indicate cardiovascular pathology, but they require professional assessment rather than a wait-and-see approach.
How I Work With Clients on Heart Health
When I take on a new male client, cardiovascular health is one of the first areas I explore. I ask about family history, current blood pressure readings if they have them, smoking status, alcohol consumption, sleep quality, and stress levels. I am not doing this to replace their GP. I am doing it because the lifestyle factors I address through coaching, including training structure, nutrition, sleep, and stress management, directly and measurably affect every single cardiovascular risk marker discussed in this article.
A client who comes to me carrying 25 kilograms of excess weight, with a blood pressure of 145 over 95, a resting heart rate of 82 beats per minute, and a cholesterol to HDL ratio of 5.2 is not just someone who wants to look better. He is a man whose cardiovascular system is under sustained stress and who will, without intervention, likely face a significant health event within the next 10 to 15 years. The work we do together, building muscle, improving aerobic fitness, restructuring nutrition, improving sleep, and reducing alcohol, addresses all of those numbers simultaneously.
I have seen blood pressure drop 15 to 20 points within 12 weeks of structured training and nutrition in clients with stage one hypertension. I have seen cholesterol to HDL ratios drop from above 5.0 to below 4.0 within six months of sustained lifestyle change. These are not unusual outcomes. They are the predictable results of applying what the research consistently shows. The body responds to the right inputs. You simply have to give it those inputs consistently enough for long enough.
If you are ready to take your cardiovascular health seriously, I would encourage you to start with two actions this week. Book a health check with your GP or use an NHS Health Check if you are eligible. And begin a structured training programme that includes both resistance training and cardiovascular exercise. Those two actions, taken now and sustained over months and years, are worth more than any supplement, any test, or any intervention you could pursue later when the options are fewer and the stakes are higher.
Work with Me
Get a personalised coaching plan built around your goals, your schedule, and your life.
Enquire NowReferences
- British Heart Foundation. (2023). Heart statistics. bhf.org.uk
- Centers for Disease Control and Prevention. (2023). Heart disease facts. cdc.gov
- Millar, P. J., et al. (2014). Evidence for the role of isometric exercise training in reducing blood pressure. Sports Medicine, 44(1), 107–116.
- Cornelissen, V. A., & Smart, N. A. (2013). Exercise training for blood pressure. Journal of the American Heart Association, 2(1), e004473.
- Kelley, G. A., & Kelley, K. S. (2012). Impact of progressive resistance training on lipids and lipoproteins. Preventive Medicine, 54(3–4), 177–183.
- Strasser, B., & Schobersberger, W. (2011). Evidence for resistance training as a treatment therapy in obesity. Journal of Obesity, 2011, 482564.
- Zhao, M., et al. (2020). Recommended physical activity and all cause and cause specific mortality. British Medical Journal, 370, m2031.
- Jenkins, D. J. A., et al. (2003). Effects of a dietary portfolio of cholesterol-lowering foods. JAMA, 290(4), 502–510.
- Appel, L. J., et al. (1997). A clinical trial of the effects of dietary patterns on blood pressure. New England Journal of Medicine, 336(16), 1117–1124.
- Rimm, E. B., et al. (1999). Folate and vitamin B6 from diet and supplements in relation to risk of coronary heart disease. JAMA, 281(23), 2140–2146.
- Ronksley, P. E., et al. (2011). Association of alcohol consumption with selected cardiovascular disease outcomes. British Medical Journal, 342, d671.
- Holmes, M. V., et al. (2014). Association between alcohol and cardiovascular disease. British Medical Journal, 349, g4164.
- Mostofsky, E., et al. (2016). Alcohol and sudden cardiac death. Journal of the American College of Cardiology, 67(9), 1015–1026.
- NHS England. (2023). NHS Health Check programme guidance. england.nhs.uk