
Body fat distribution men women is one of the most important and least discussed topics in the entire fat loss conversation. Most people think about body fat in simple terms: you have too much of it or you do not. But the reality is that where your body stores its fat is just as significant as how much of it you carry. Men and women store fat in fundamentally different ways, driven by hormones, genetics, and biology that have been shaped over hundreds of thousands of years of human evolution. These differences are not cosmetic curiosities. They have direct, measurable implications for your metabolic health, your risk of chronic disease, and the way you should approach your nutrition and training.
I work with men and women across every age group and every dietary background, from meat eaters to vegetarians to vegans. One of the first things I explain to every new client is that their body is not a blank canvas. It has a blueprint, shaped by their sex, their hormones, and their individual physiology, and the approach I build for them needs to respect that blueprint. A training and nutrition plan that works brilliantly for a 35 year old man will not work the same way for a 50 year old woman going through menopause. Understanding the biology behind sex differences in fat storage is the first step towards building a programme that actually works for your body.
The Biology: Why Men and Women Store Fat in Different Places
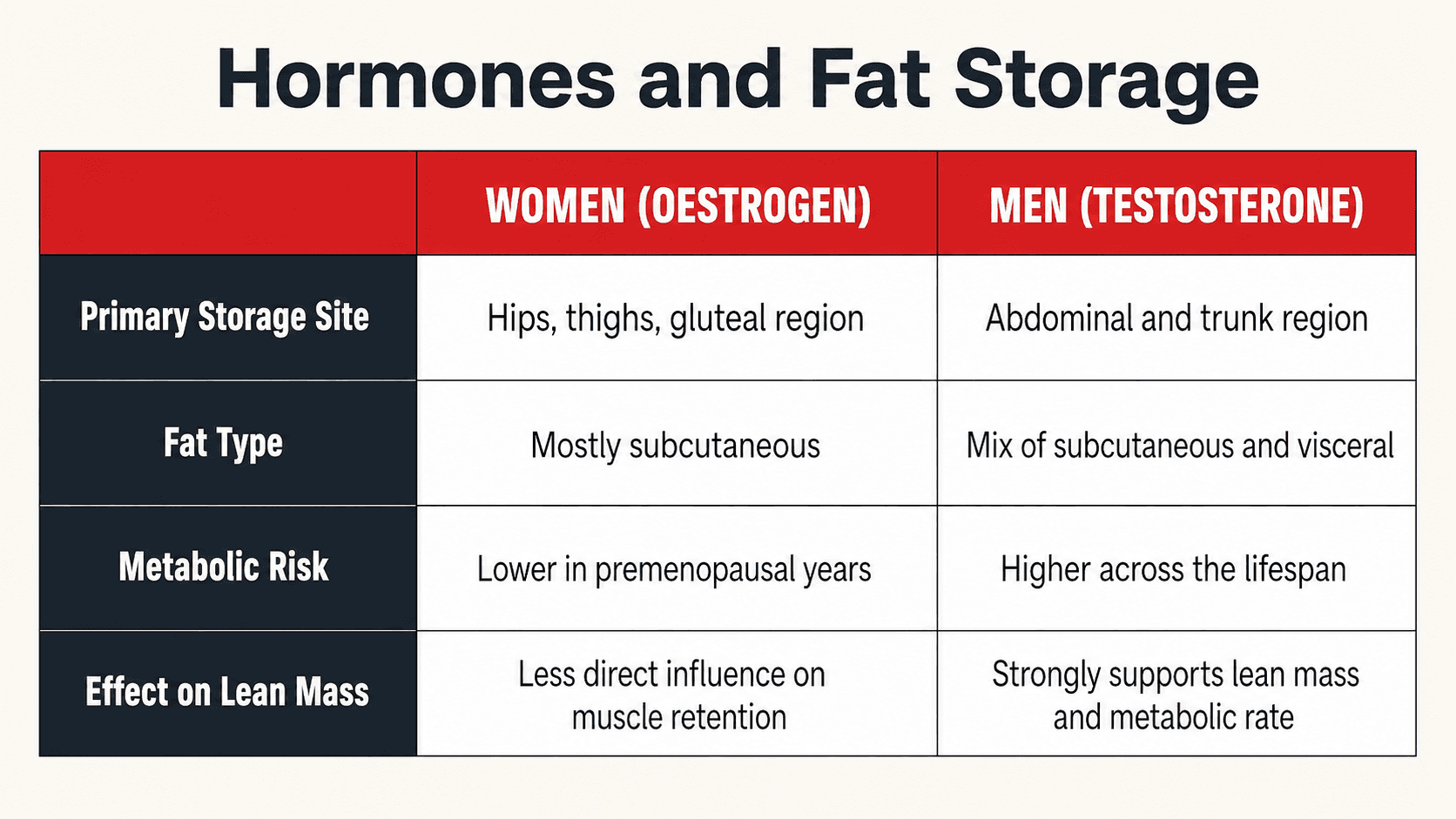
The primary driver of sex differences in fat distribution is hormones, specifically oestrogen and testosterone. These two hormones do not just influence reproductive function. They exert powerful effects on where and how your body deposits fat, how metabolically active that fat is, and how it responds to calorie restriction and exercise.
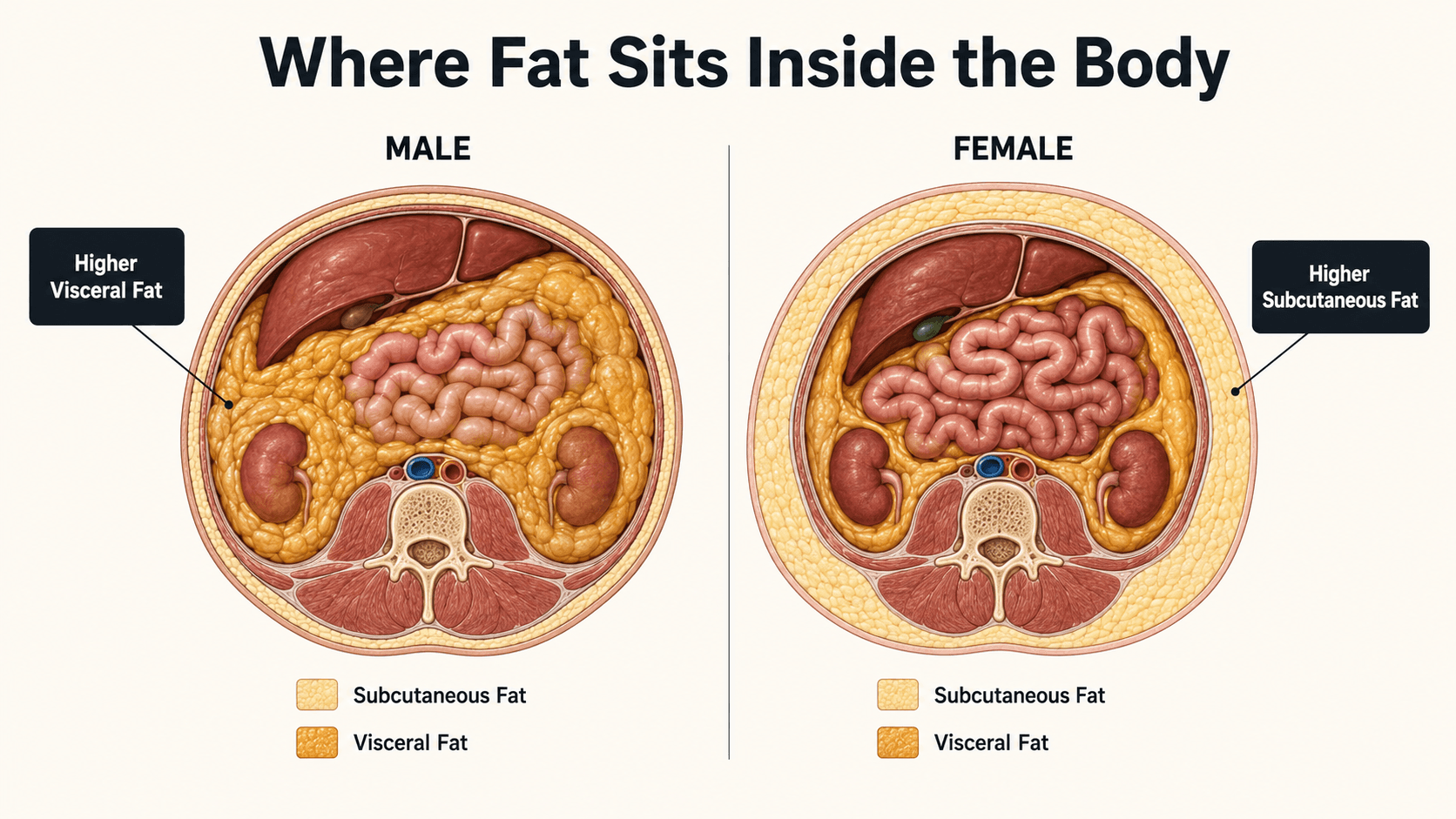
Women, particularly premenopausal women, tend to store fat preferentially in subcutaneous depots in the hips, thighs, and buttocks. This is known as a gynoid pattern and it is driven primarily by oestrogen. Oestrogen promotes the activity of lipoprotein lipase in lower body fat tissue, essentially directing dietary fat towards storage in the gluteofemoral region (1). This lower body fat is largely subcutaneous, meaning it sits under the skin rather than around the internal organs. It is metabolically less dangerous than visceral fat and in some contexts may even be protective, acting as a buffer for excess energy that keeps fat away from the liver, pancreas, and other organs where it causes the most damage (2).
Men follow a very different pattern. Testosterone does not provide the same protective redirection of fat towards the lower body. Instead, men tend to accumulate fat in the abdominal region, both subcutaneously and viscerally. This is known as an android pattern. Visceral fat, the fat stored deep inside the abdominal cavity around the internal organs, is metabolically active tissue that releases inflammatory cytokines, free fatty acids, and hormones directly into the portal circulation. It impairs insulin signalling, drives hepatic insulin resistance, and creates a chronic inflammatory state that accelerates the progression towards type 2 diabetes and cardiovascular disease (3). This is the primary reason men develop metabolic disease at lower levels of total body fat and at younger ages than premenopausal women.
A large cross-sectional study using data from the National Health and Nutrition Examination Survey confirmed these patterns, showing that testosterone in men was strongly and positively associated with lean body mass and negatively associated with fat mass, while in women oestradiol levels were the primary hormonal determinant of body composition (4). The study used dual energy X-ray absorptiometry and mass spectrometry for precise measurement, confirming that these hormonal influences are robust and measurable at a population level.
Menopause Changes Everything for Women
One of the most significant shifts in fat distribution that I see in my coaching practice occurs in women during and after menopause. When oestrogen levels decline, the protective effect that directed fat towards the lower body begins to disappear. Fat distribution shifts away from the hips and thighs and towards the abdomen. Post-menopausal women begin to accumulate more visceral fat, and their metabolic risk profile starts to resemble that of men.
Research confirms that this shift is specifically related to oestrogen deficiency rather than ageing alone. While total body fat may increase with age in both sexes, the redistribution of fat from subcutaneous peripheral depots to visceral abdominal depots is driven by the hormonal changes of menopause (5). Women who receive post-menopausal hormone therapy see an age-adjusted decrease in visceral fat compared to those who do not (5). This tells us something important: the fat redistribution is hormonally mediated and not simply an inevitable consequence of getting older.
For the women I work with who are in their late 40s, 50s, and beyond, this is not just academic information. It changes the way I structure their nutrition and training. The protective hormonal environment they relied on for decades is changing, and their approach needs to change with it. Resistance training becomes even more critical because it directly improves insulin sensitivity and supports metabolic health independently of fat loss. Protein intake needs to be higher because ageing muscle becomes less responsive to anabolic signals, a phenomenon known as anabolic resistance (6). Waist circumference monitoring becomes essential because the scale may not move much while visceral fat quietly accumulates. I have worked with post-menopausal women who gained very little weight on the scale but whose waist circumference crept up by several centimetres over a year. Without measurement, that shift would have gone completely undetected.
Low Testosterone and Fat Accumulation in Men
Men face their own hormonal challenges when it comes to fat storage. Testosterone levels decline gradually with age, typically by about 1 to 2 percent per year after the age of 30. This is sometimes referred to as andropause, although it is a far more gradual process than female menopause. As testosterone declines, men tend to accumulate more visceral fat, lose muscle mass, and develop worsening insulin sensitivity.
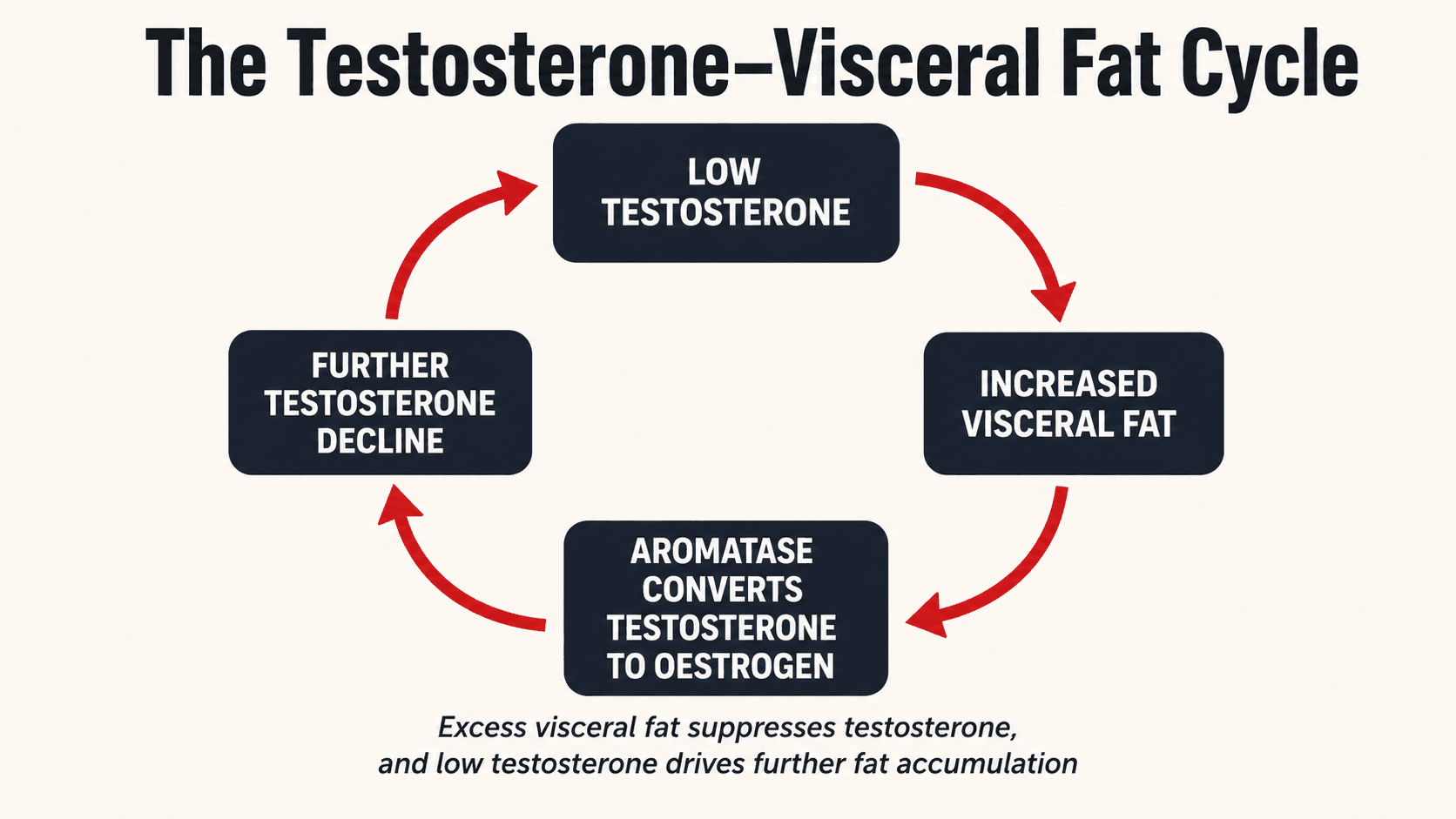
The relationship between testosterone and visceral fat in men is bidirectional and this is a critical point. Low testosterone promotes visceral fat accumulation, but excess visceral fat also suppresses testosterone production. Adipose tissue contains the enzyme aromatase, which converts testosterone to oestradiol. The more visceral fat a man carries, the more testosterone is converted to oestrogen, further lowering testosterone levels and creating a self-reinforcing cycle of fat gain and hormonal disruption (7). This is why I see so many men in their 40s and 50s who have gradually gained abdominal fat over a decade and simultaneously feel less energetic, less motivated, and less able to build muscle. The fat is not just a cosmetic issue. It is actively undermining their hormonal health.
The good news is that this cycle is breakable. Research has consistently shown that fat loss, particularly visceral fat loss, through calorie restriction and exercise leads to significant increases in testosterone levels in overweight and obese men (7). You do not necessarily need testosterone replacement therapy to improve your hormonal profile. In many cases, losing the visceral fat that is suppressing your testosterone in the first place is enough to restore levels to a healthier range. This is something I have seen repeatedly in my male clients: as their waist circumference comes down and their body composition improves, their energy, mood, and training performance improve alongside it.
Why These Differences Should Change How You Train and Eat
Understanding the biology of sex-specific fat distribution is not just interesting. It should directly influence your approach to fat loss. Here is why.
For men, the priority is typically visceral fat reduction. The fat that poses the greatest health risk is the fat around the organs, and the most effective interventions for reducing it are well established. A calorie deficit, resistance training, and aerobic exercise all significantly reduce visceral fat, with a clear dose-response relationship: the more energy you expend, the greater the reduction (8). Resistance training is particularly important for men because it directly supports testosterone production and muscle mass retention, both of which decline with age and both of which are essential for long-term metabolic health.
For premenopausal women, fat loss may be slower and the body may preferentially hold onto lower body fat for longer. This is not a failure of the programme. It is biology. Lower body subcutaneous fat is more resistant to mobilisation than visceral fat, partly because it has lower blood flow and a different receptor profile. Women should not panic if their hips and thighs are the last areas to lean out. That fat is metabolically safer than abdominal fat and will reduce with sustained adherence to a calorie deficit and training programme over time.
For post-menopausal women, the approach needs to shift. The declining oestrogen environment means visceral fat is now a real and growing threat. Resistance training at least two to three times per week is essential, not optional. Protein intake should be at the higher end of recommendations, around 1.6 to 2.2 grams per kilogram of body weight per day, to counteract anabolic resistance. Whole food sources like tofu, tempeh, lentils, chickpeas, eggs, fish, lean meats, soy protein, and pea protein should form the foundation of every meal. Monitoring waist circumference becomes as important as monitoring body weight.
PCOS, Hyperandrogenism, and Fat Distribution in Women
Polycystic ovary syndrome is one of the most common endocrine disorders affecting women of reproductive age, and it has a direct and significant impact on fat distribution. Women with PCOS typically have elevated androgen levels, a condition known as hyperandrogenism, which shifts their fat storage pattern away from the typical female gynoid pattern and towards a more android pattern with increased visceral fat accumulation. This is associated with greater insulin resistance, higher risk of type 2 diabetes, and a more adverse metabolic profile compared to women without PCOS (9).
I have coached many women with PCOS through successful body transformations. The approach needs to be tailored: insulin sensitising strategies are important, which means prioritising resistance training, managing carbohydrate quality rather than eliminating carbohydrates entirely, ensuring adequate protein, and creating a sustainable calorie deficit. Women with PCOS often respond well to higher protein, moderate carbohydrate approaches that emphasise low glycemic index sources such as oats, sweet potatoes, lentils, basmati rice, and legumes. It takes longer and requires more patience, but the results are absolutely achievable.

Top Tips: What You Can Implement Today
Based on everything covered in this article, here are actionable steps you can take immediately regardless of your sex, your age, or your dietary preferences.
Measure your waist circumference today and write it down. Use a tape measure at the midpoint between your lowest rib and the top of your hip bone. For men, aim to keep this below 94 cm. For women, below 80 cm. If you are above these thresholds, reducing your waist circumference should be a primary health goal. Track it monthly alongside your body weight.
Do not rely on BMI alone to assess your health. BMI tells you nothing about where your fat is stored or how much of your weight is muscle versus fat. Request a full metabolic blood panel from your GP, including fasting glucose, HbA1c, fasting insulin, a full lipid panel, and liver function tests. These markers tell you far more about your metabolic health than your weight ever will.
Prioritise resistance training at least two to three times per week. This applies to both men and women. Resistance training builds and preserves lean muscle mass, improves insulin sensitivity, supports hormonal health, and is one of the most effective tools for reducing visceral fat. It is non-negotiable in any serious body composition programme.
Set your protein intake at 1.6 to 2.2 grams per kilogram of body weight per day. Whether you eat meat, are vegetarian, or are fully vegan, this target is achievable and essential. Build meals around high quality protein sources: chicken, fish, eggs, tofu, tempeh, seitan, lentils, chickpeas, soy protein, pea protein, Greek yoghurt, or dairy alternatives. Protein supports muscle retention during fat loss, improves satiety, and has a higher thermic effect than carbohydrates or fat.
If you are a woman over 45, pay extra attention to your waist circumference and your strength. The hormonal changes of menopause shift fat storage towards the abdomen. Resistance training and adequate protein become even more important. Do not accept increasing waist circumference as an inevitable part of ageing. It is a modifiable risk factor and you have the power to control it.
If you are a man carrying weight around your midsection, treat it as a health priority, not a cosmetic one. Visceral fat actively suppresses testosterone, drives insulin resistance, and promotes systemic inflammation. Losing abdominal fat through a structured calorie deficit and training programme will improve your hormones, your blood work, and your quality of life. This is not about vanity. This is about longevity.
Walk more. Aim for 8,000 to 10,000 steps per day. Daily walking increases total energy expenditure without the recovery cost of intense training. It is one of the simplest, most sustainable, and most effective tools for supporting fat loss and improving metabolic health, and it is completely free.
If you have PCOS, do not assume fat loss is impossible. It is harder, not impossible. Focus on resistance training, protein, and low glycemic carbohydrate sources. Work with a coach who understands the condition. The results will come.
The Bottom Line
Men and women are biologically different in how and where they store body fat, and these differences carry meaningful implications for health, disease risk, and the optimal approach to fat loss. Oestrogen directs fat towards the lower body in premenopausal women, offering a degree of metabolic protection. Testosterone supports lean mass and limits fat accumulation in men, but its decline with age contributes to visceral fat gain. Menopause removes the hormonal protection women have relied on for decades, shifting fat towards the abdomen and increasing metabolic risk. PCOS disrupts the typical female pattern and increases visceral fat in younger women. Understanding these patterns is not optional if you are serious about your health. It is the foundation on which an effective, personalised fat loss programme should be built.
If you want a programme designed around your body, your hormones, your age, and your dietary preferences, get in touch through trperformancecoaching.com. I work one-to-one with clients online globally. Whether you eat meat, are vegetarian, vegan, or somewhere in between, whether you are a man dealing with rising abdominal fat and declining energy, a woman navigating menopause, or someone managing PCOS, I will build an approach that works for your biology, not against it. Your body is not a problem to fight. It is a system to understand and work with.
Work with Me
Get a personalised coaching plan built around your goals, your schedule, and your life.
Enquire NowReferences
- Fried SK, Lee MJ, Karastergiou K. Shaping fat distribution: new insights into the molecular determinants of depot- and sex-dependent adipose biology. Obesity. 2015; 23(7): 1345-1352.
- Manolopoulos KN, Karpe F, Frayn KN. Gluteofemoral body fat as a determinant of metabolic health. International Journal of Obesity. 2010; 34(6): 949-959.
- Tchernof A, Després JP. Pathophysiology of human visceral obesity: an update. Physiological Reviews. 2013; 93(1): 359-404.
- Hirsch KR, Grossmann M, Engeli S, et al. Differential association of sex hormones with metabolic parameters and body composition in men and women from the United States. Journal of Clinical Medicine. 2023; 12(14): 4783.
- Palmer BF, Clegg DJ. The sexual dimorphism of obesity. Molecular and Cellular Endocrinology. 2015; 402: 113-119.
- Burd NA, Gorissen SH, van Loon LJC. Anabolic resistance of muscle protein synthesis with aging. Exercise and Sport Sciences Reviews. 2013; 41(3): 169-173.
- Grossmann M. Low testosterone in men with type 2 diabetes: significance and treatment. Journal of Clinical Endocrinology and Metabolism. 2011; 96(8): 2341-2353.
- Verheggen RJHM, Maessen MFH, de Groot DRMJ, Hermus ARMM, Eijsvogels TMH, Hopman MTE. Dose-response effects of exercise and caloric restriction on visceral adiposity in overweight and obese adults. British Journal of Sports Medicine. 2023; 57(16): 1035-1041.
- Escobar-Morreale HF. Polycystic ovary syndrome: definition, aetiology, diagnosis and treatment. Nature Reviews Endocrinology. 2018; 14(5): 270-284.
